


The CDC reports 14 with Salmonella Senftenberg in 12 States linked to Jif peanut butter. Arkansas (1), Georgia (2), Illinois (1), Massachusetts (1), Missouri (1), Ohio (1), North Carolina (1), New York (1), South Carolina (1), Texas (2), Virginia (1), and Washington (1).
However, as the CDC says, “the true number of sick people in an outbreak is likely much higher than the number reported, and the outbreak may not be limited to the states with known illnesses. This is because many people recover without medical care and are not tested for Salmonella.”
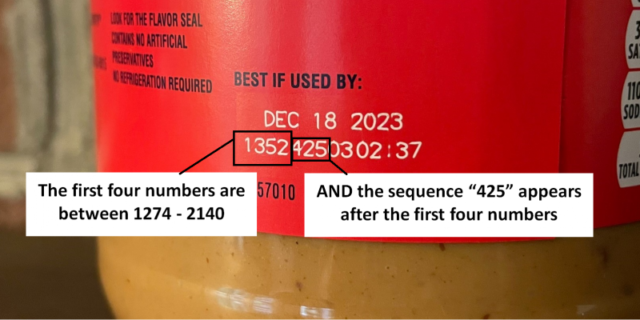
Lot code numbers 1274425 through 2140425, with “425” at the end of the first 7 numbers.
Here is the current recall list – it will grow.
Thanks to eFoodAlert.
The CDC estimates Salmonella bacteria cause about 1.35 million infections, 26,500 hospitalizations, and 420 deaths in the United States every year. Food is the source for most of these illnesses.
If you have the above symptoms, stay hydrated and seek medical attention. Ask your treating physician to order a stool culture to test to see if you have been infected with the outbreak strain of Salmonella Senftenberg.
If you have leftover Jif, consider having a lab test it for Salmonella Senftenberg.
Salmonella: Marler Clark, The Food Safety Law Firm, is the nation’s leading law firm representing victims of Salmonella outbreaks. The Salmonella lawyers of Marler Clark have represented thousands of victims of Salmonella and other foodborne illness outbreaks and have recovered over $800 million for clients. Marler Clark is the only law firm in the nation with a practice focused exclusively on foodborne illness litigation. Our Salmonella lawyers have litigated Salmonella cases stemming from outbreaks traced to a variety of foods, such as cantaloupe, tomatoes, ground turkey, salami, sprouts, cereal, peanut butter, and food served in restaurants. The law firm has brought Salmonella lawsuits against such companies as Cargill, ConAgra, Peanut Corporation of America, Sheetz, Taco Bell, Subway and Wal-Mart.
If you or a family member became ill with a Salmonella infection, including Reactive Arthritis or Irritable bowel syndrome (IBS), after consuming food and you’re interested in pursuing a legal claim, contact the Marler Clark Salmonella attorneys for a free case evaluation.
Additional Resources:
What we know: There have been four sick with two dead from Cronobacter sakazakii linked to Abbott’s manufacturing plant.
Now the House and Senate are set to ask questions of the Industry and FDA about how the outbreak happened and how it impacted the supply of infant formula.
Formula Safety and Supply: Protecting the Health of America’s Babies – Wednesday, May 25 at 11am, House Energy and Commerce Committee
The Infant Formula Crisis – Wednesday, May 25 at 2pm, House Committee on Appropriations
Infant Formula Crisis: Addressing the Shortage and Getting Formula On Shelves – Thursday, May 26 at 10:30am, U.S. Senate Committee on Health, Education, Labor & Pensions
Here is a preview of the FDA’s position See full testimony – FDA Testimony ECOI Infant Formula 5.25.2022 final:
TESTIMONY OF
ROBERT M. CALIFF, M.D. COMMISSIONER OF FOOD AND DRUGS
FRANK YIANNAS, M.P.H.
DEPUTY COMMISSIONER, FOOD POLICY AND RESPONSE
SUSAN T. MAYNE, PH.D.
DIRECTOR, CENTER FOR FOOD SAFETY AND APPLIED NUTRITION
FOOD AND DRUG ADMINISTRATION DEPARTMENT OF HEALTH AND HUMAN SERVICES
BEFORE THE
SUBCOMMITTEE ON OVERSIGHT AND INVESTIGATIONS COMMITTEE ON ENERGY AND COMMERCE
U.S. HOUSE OF REPRESENTATIVES
FORMULA SAFETY AND SUPPLY: PROTECTING THE HEALTH OF AMERICA’S BABIES
MAY 25, 2022
RELEASE ONLY UPON DELIVERY
Introduction
Chair DeGette, Ranking Member Griffith, and members of the Subcommittee, thank you for inviting us here today to testify before you on supply disruptions in infant formula. We have all seen the images of empty store shelves and heard the stories of parents of kids unable to find the food their children need to survive. This situation is unacceptable. The staff at the U.S. Food and Drug Administration (FDA or the Agency) feel this not just as public servants whose job it is to ensure that these critical products are safe and nutritious, but also as parents and grandparents. Our top priority now is addressing the dire need for infant formula in the U.S. market, and our teams are working night and day to help make that happen.
At the same time, we have begun an after-action review to evaluate our own performance. We appreciate the opportunity to discuss conditions at the Abbott Nutrition facility in Sturgis, Michigan, which led to the recall that contributed to the current supply disruptions; our infant formula supply chain monitoring and mitigation efforts; and additional tools necessary if we are to prevent, monitor, and mitigate any future infant formula supply disruptions.
Inspection of Abbott Nutrition’s Sturgis, Michigan, Facility
On September 20, 2021, FDA learned of a Cronobacter infection in an infant who reportedly consumed powdered infant formula produced at Abbott Nutrition’s Sturgis, Michigan, facility. FDA immediately reported this case to Abbott Nutrition and immediately followed up on the complaint, including testing formula associated with this case complaint. No Cronobacter was recovered from the product after FDA testing.
On November 17, 2021, FDA received a complaint involving an infant with Salmonella infection. FDA and our partners at the Centers for Disease Control and Prevention (CDC) eventually determined this event was unrelated to the other cases.
FDA received the second complaint involving an infant with Cronobacter infection on December 1, 2021. We again collected intact samples of powdered formula; no Cronobacter was recovered. We also notified Abbott Nutrition about this case.
Because Cronobacter is not a nationally reportable disease, isolates of the pathogens had not routinely undergone genomic analyses, as would occur with pathogens like Salmonella. In 2021 there was no genetic evidence available for us to know if these two cases from 2021 were linked by whole genome sequencing.
But given the two case complaints and the potential severity of Cronobacter infections, along with a complaint from a former employee at the Sturgis facility, on December 6, 2021, FDA initiated inspectional planning for a for-cause inspection at the Sturgis facility with an anticipated inspection date in early January 2022. We notified Abbott Nutrition of the planned inspection on December 30, 2021. Abbott Nutrition responded by notifying FDA of approximately a dozen COVID-19-positive employees in its facility. Although we delayed our inspection temporarily because of these COVID-19 infections, FDA commenced our inspection on January 31, 2022.
FDA received a third report of an infant Cronobacter illness on January 11, 2022, while the facility’s COVID-19 outbreak delayed FDA’s inspection. Again, FDA tested product associated with this illness, found no Cronobacter, and notified Abbott Nutrition.
FDA learned of a fourth case of Cronobacter infection on February 17, 2022, the date on which Abbott Nutrition initiated a voluntary recall and FDA issued a consumer advisory.
Infants in all four cases were hospitalized, and Cronobacter may have contributed to deaths in two cases. All of the infants are reported to have consumed powdered infant formula produced at Abbott Nutrition’s Sturgis facility. The Agency investigated each complaint and analyzed product from the consumers’ homes when available. FDA also notified Abbott Nutrition after receiving each complaint.
The CDC receives reports on foodborne disease outbreaks from state, local, and territorial health departments. On average, CDC receives two to four Cronobacter case reports annually; however, because Cronobacter infection is not reportable in most states, the total number of cases that occur in the United States each year is not known. Thus, the four cases that came to our attention between September 20, 2021, and February 17, 2022, raised concerns. Despite this very unusual combination of events, we do not have definitive evidence proving that insanitary conditions of the Sturgis facility actually caused the Cronobacter illnesses of these infants.
We have included this timeline in Appendix A, and we have processes under review to develop better systems within FDA.
In sum, awareness of the four Cronobacter cases offered an evolving fact pattern, leading us to initiate a for-cause inspection, but our inspection dramatically altered the fact pattern.
Sanitary environmental conditions and well-maintained equipment are the most basic, minimal conditions needed for a manufacturer to produce dry powdered infant formula that is free of bacterial contamination. The FDA inspection team observed significant operational deficiencies in Abbott Nutrition’s Sturgis facility during the January 2022 inspection. The totality of evidence obtained during our inspection caused FDA to conclude that infant formulas produced at this plant were produced under insanitary conditions and may be contaminated with Cronobacter. We based our conclusions on the following evidence:
FDA investigators collected numerous product and environmental samples during the inspection. Product samples FDA collected at Abbott Nutrition’s Sturgis facility and analyzed for Cronobacter tested negative. It is well documented in the scientific literature, however, that end product testing is unlikely to detect low levels of contamination. In contrast, five environmental subsample surface swabs collected from the facility tested positive for Cronobacter sakazakii; four of these instances of contamination were detected by FDA-initiated testing, and one was detected through simultaneous firm-initiated testing. The positive Cronobacter sakazakii environmental samples collected at Abbott Nutrition’s Sturgis facility have been analyzed using whole genome sequencing, revealing five different strains of Cronobacter sakazakii. While none of these environmental samples matched the limited (two) clinical samples from infants ill with Cronobacter, these findings remain a serious concern, as environmental sources of Cronobacter in infant formula manufacturing plants have been identified as one of the most likely sources of contamination.
As soon as the Agency received these positive environmental sampling results in February 2022, we communicated with Abbott Nutrition about the need for the firm to issue a voluntary recall. Abbott Nutrition voluntarily ceased production at the Sturgis facility two days prior to the recall, and FDA supported this decision given the insanitary conditions at the facility. On February 17, 2022, we issued a public communication advising consumers not to use the affected products. Abbott Nutrition initiated a voluntary recall the same day.
Insanitary conditions of this kind are unacceptable in all food manufacturing facilities, but especially in areas producing dry powdered formulas that serve as the sole source of nutrition for infants. Finding pathogens in finished product during routine testing also generally indicates a potentially serious loss of sanitary process control during manufacturing. FDA would expect any manufacturer with a robust quality assurance program to identify and quickly take corrective action when such conditions are present.
FDA knew that restarting the Sturgis, Michigan, facility was critical, because it was one of three plants run by a company with the largest market share, and many of its specialty formula products cannot be quickly manufactured at other facilities. We also became aware that Abbott Nutrition lacked a contingency plan to produce its lines of specialty metabolic and amino acid formulas that serve as a sole source of nutrition for thousands of infants with metabolic disorders. We lost confidence that Abbott Nutrition had the appropriate safety and quality culture and commitment to fix these problems quickly. FDA was left with limited options. Given the market share that Abbott Nutrition had for regular and critically needed specialty metabolic and amino acid formulas, FDA decided to negotiate a consent decree with the company rather than seeking a court order of permanent injunction through a contested process. A consent decree was the best option, giving FDA more control over the outcome, and was more likely to result in a safe resumption of operations by Abbott Nutrition at the Sturgis facility.
With the urgent public health need in mind, FDA, along with the U.S. Attorney’s Office for the Western District of Michigan, moved as quickly as possible through the negotiation process. In fact, the process here was shorter than it often is for obtaining a consent decree. FDA made clear its expectations for a safe reopening of the facility. Even still, because it was a negotiation process with a regulated firm, the U.S. government did not completely control the timeline. Moreover, FDA’s negotiations needed to be informed by our inspection of the Sturgis facility, which did not close until March 18, 2022, to ensure that the consent decree would fully address all observed violations.
FDA’s and U.S. Government Actions to Increase the Supply of Specialty Metabolic Formulas
When we talk about the infant formula supply chain, we really need to consider multiple supply chains, including, but not limited to, the supply of infant formula for healthy infants, another for infants with allergies and/or medical conditions who need hypoallergenic amino acid formulas, and another for infants who have very serious medical conditions, such as inborn errors of metabolism, and require unique specialty metabolic formulas. Abbott Nutrition dominates the market for many of the amino acid-based and metabolic formulas. Unfortunately, the only site where Abbott Nutrition produces these critical products is the Sturgis plant. Thus, the Agency immediately had to consider the potential impact a recall of these specialty formulas could have on infant health.
FDA decided to exempt specialty metabolic products from the recall and required that the current stock of these formulas in storage would be subject to third-party review before release. Some of the infants who were using these non-recalled products could potentially be switched to comparable products, but transitioning is not always well tolerated or possible and thus requires clinical input from the child’s health care provider. For this reason, we coordinated with groups such as the American Academy of Pediatrics, Genetic Metabolic Dietitians International, and the Society of Inherited Metabolic Disorders so providers would be prepared to advise their patients whether switching products was appropriate. We also coordinated with the U.S. Department of Agriculture’s (USDA) Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), and made them aware of the pending recall in advance of it occurring. To help support supply chains, our infant formula team had to determine for each of these products what comparable products might exist from other infant formula manufacturers and request that they increase production of these products as much as possible. These efforts included seeking available inventory outside of the domestic market.
FDA worked with Abbott Nutrition to identify and prioritize specialty and metabolic formulas and asked Abbott Nutrition to establish a process to provide these formulas to those in need on a case-by-case basis. After the third-party audit concluded, Abbott Nutrition began releasing these critical products on a case- by-case basis. In these circumstances, the benefit of allowing caregivers, in consultation with their healthcare providers, to access these products may outweigh the potential risk of bacterial infection. FDA determined that the case-by-case release of these priority products is the best solution prior to resuming production of them at Abbott Nutrition’s Sturgis facility. Since Abbott Nutrition did not have a plan or any capability to produce these critical, lifesaving products at another of their facilities, case-by-case release was the only option. FDA continues to use all levers we have, including Operation Fly Formula, to be able to increase the supply of these formulas, which come from an even more limited set of manufacturers than general infant formula. The first airlifts of infant formula as part of Operation Fly Formula are amino acid and hypoallergenic hydrolyzed formulas that are most critically needed. We note that having access to good data on the availability of specialty and metabolic formulas is challenging; measures useful to assess the supply of general formula such as those from Information Resources Inc. (IRI) (discussed below), are not informative for these products, as they are not always sold in traditional retail settings.
FDA’s Work with Partners to Increase the Broader Infant Formula Supply
The United States was facing infant formula supply chain stress even before the Abbott Nutrition recall began on February 17, 2022. Abbott Nutrition’s voluntary recall and subsequent voluntary cessation of operations at its Sturgis plant in February further destabilized the infant formula supply chain. Prior to the voluntary recall of several infant formula products produced at the Abbott Nutrition facility, FDA was working to address supply chain issues associated with the pandemic, including those impacting the infant formula industry. Our efforts to help support an all-of-government supply chain response included regular engagement with the Infant Nutrition Council of America (INCA), and its members, to identify challenges they were facing. Beginning immediately after the recall in February, this work greatly intensified, and the Agency has been working extensively with Abbott Nutrition and other manufacturers to bring safe products to the U.S. market as quickly as possible.
FDA’s intra-agency group includes experts from the Office of Food Policy and Response (OFPR) and the Center for Food Safety and Applied Nutrition (CFSAN). They began evaluating infant formula supply chain implications prior to the recall, met with USDA, and ensured that U.S. government supply chain partners were engaged at the highest levels. FDA and USDA, as co-leads for Food and Agriculture Sector Risk Management, provided regular updates to the White House regarding overall supply chain concerns, including information about infant formula. Since the first day, FDA has worked tirelessly with U.S. government partners to mitigate the supply chain disruption for both regular and specialty formulas.
It is important to understand that only facilities experienced in and already producing infant formula and specialty metabolic products are in a position to make products that would not pose significant health risks to consumers. Infant formulas for healthy, full-term infants are complex in terms of formulation, processing, and other considerations to achieve required levels of 30 different nutrients and to avoid excessive levels of 10 nutrients that can be toxic when levels are too high. Formulas for low birth weight or premature infants, or those with serious health conditions, are even more complex; for example, hypoallergenic formulas need to be manufactured to ensure cross-contact with other formulas made in a facility does not occur.
FDA continues taking key steps to help increase the supply of infant formula in the United States. FDA is leveraging all tools at our disposal to support the supply of infant formula products:
In broader whole-of-government efforts, agencies are working together to improve the supply of infant formula to American families by:
FDA has been working closely with all major infant formula manufacturers to mitigate supply disruption. All manufacturers already in the U.S. market have increased production to capacity. However, FDA lacks authority, resources, or dedicated staff to predict, detect, and respond to supply chain issues for infant formula and medical foods – although we have requested authority to do so since 2020, including in our fiscal year (FY) 2022 and FY 2023 budget requests. FDA developed this legislative proposal because we were well aware that the U.S. infant formula supply chain was dominated by a small number of actors with only a handful of manufacturing facilities – making it at high risk for disruption by any single event or stressor. Even without the authorities to compel submission of supply chain data, FDA took numerous steps to request these data and shore up supply to the extent we received cooperation of firms.
Following FDA’s efforts, the major infant formula manufacturers are producing at increased capacity and have been further optimizing their lines to produce more infant formula to meet current demand. In the month of April, consumers purchased more infant formula than they did in the four weeks prior to the recall, which is a good indication that powdered infant formula availability is headed in the right direction. Data from IRI show nearly 80 percent in-stock rates for the week ending May 15, 2022, (compared to 89 to 90 percent in-stock rates before the Abbott Nutrition recall; see figure 1). This means that if a local supermarket normally carries 50 different infant formula products, an 80 percent in-stock rate translates to 40 of those 50 product types being available. But we understand – as parents and grandparents ourselves – that many have been unable to access the products they need and that they are understandably frustrated and anxious.

While in-stock rates have dropped gradually because of Abbott Nutrition’s inability to resume production as quickly as we all would like, there are some positive trends because of FDA’s call to action to the rest of the industry. National infant formula sales by volume for the most recent four weeks of data through May 8, 2022, increased 12 percent compared to the four weeks prior to the recall (see figure 2). And national infant formula sales by unit increased 5 percent for the most recent four weeks of data through May 8, 2022, compared to the four weeks prior to the recall (see figure 3).

Through our weekly intensive discussion with manufacturers, we also know that all producers that supply the U.S. market have already stepped up to the challenge and are telling us they are producing at an expanded capacity. For example, Nestle Gerber increased the amount of its infant formula available to consumers by approximately 50 percent in March and April, and Reckitt is supplying more than 30 percent more product so far this year.
What these data tell us collectively is that while there is more product being produced and sold, it is of less variety than prior to the recall. These metrics also indicate that we are on a positive trajectory. However, we know that one parent not being able to find the products they want is one parent too many, and we, also, have seen the photos of empty shelves and heard of the stressful stories of parents having to work extra hard to find product. This is unacceptable.
Importantly, we know that some data suppliers who use less standardized metrics have reported lower in- stock rates, and we believe those news reports, recited without validation, may have exacerbated the situation in recent weeks. Throughout the pandemic, retailers have experienced a new type of consumer behavior – which we can appreciate and understand – where consumers may purchase additional units to ensure they can stock their pantries, because of a loss in confidence that their desired products will be available during their next grocery shopping trip. And when it comes to ensuring their infants have access to a sole source of nutrition, this behavior is understandable.
As discussed above, data available to FDA show that volume sales of infant formula, as a category, are currently higher than they were before the Abbott Nutrition recall. However, there have been dramatic shifts in which products (e.g., brand, type, and size) are being sold, and the recent increases in consumption create empty shelves that require further ramp up of supply. In addition, there are significant concerns related to the availability of certain specialty formula products, such as amino acid-based products and formulas for individuals with inborn errors of metabolism – these are products on which FDA has been especially focused. Indeed, the availability of specialty and metabolic formulas remains a fluid and evolving situation.
The Agency’s best current assessment is that with all of the current actions, and the potential for Abbott Nutrition’s Sturgis facility to resume production safely in the near term, the supply of infant formula will continue to improve over the next several weeks. In the meantime, FDA is encouraged to see that as of early May, the amount of infant formula sold in the United States continues to rise.
On May 16, 2022, the U.S. District Court for the Western District of Michigan entered a consent decree of permanent injunction between FDA and Abbott Nutrition, as well as three Abbott Nutrition principals. Under the consent decree, Abbott Nutrition has agreed to take corrective actions following FDA’s inspection of its Sturgis, Michigan, facility. The consent decree obligates Abbott Nutrition to take actions that are expected to ultimately result in an increase of infant formula products, while ensuring that the company undertakes certain actions that would ensure safe powdered infant formula is produced at the facility. When the company restarts production at this facility, it must conform with the provisions of the consent decree and meet FDA food safety standards. If contamination is identified, the company must notify FDA, identify the source of the problem, and conduct a root-cause investigation before resuming production.
Modernizing Infant Formula Safety and Supply Chain Security
We take seriously our duty to prevent and respond to foodborne illnesses and food contamination events. FDA will be conducting an evaluation of our response to this incident and determine what additional steps should be taken to ensure the maximum effectiveness of Agency programs and policies related to infant formula and medical food complaints, illnesses, and recalls.
More than 3.5 million babies are born in the United States each year, many of whom rely on formula at some point as their sole source of nutrition. FDA has nine staff devoted to reviewing infant formula premarket submissions for safety and nutrition. Even before the voluntary recall and production halt at Abbott Nutrition’s Sturgis facility, FDA’s infant formula staff faced increased workload due to COVID- 19 supply chain issues and increased product innovation in the infant formula industry. Furthermore, the war in Ukraine has caused a disruption in the supply of sunflower oil, an ingredient in many formulas, which has further increased FDA’s review responsibilities as manufacturers assess their supply chains and needs to reformulate product. Recent actions to increase imports will also increase FDA’s workload, as the review team must review incoming applications and collaborate with the food safety team to ensure that these products are both safe and nutritionally adequate.
The wide-reaching impacts of a recall from a single infant formula manufacturing facility underscore the risks and vulnerabilities in the supply chain when production is consolidated among few major manufacturers utilizing few manufacturing facilities. Building resiliency across the infant formula supply chain will better enable the industry to withstand any future disruptions without a significant breakdown in supply. To this end, we are exploring additional mechanisms to incentivize flexibility and redundancy of the infant formula supply chain infrastructure to increase resiliency in the infant formula industry over the long term. Recommendations from the White House’s 100-day supply chain review report1 with regard to pharmaceutical and active pharmaceutical ingredient supply chain resiliency may prove insightful here. In partnership with other agencies across the U.S. government, we also hope to initiate a broad dialogue on how contracting models for these products could be enhanced to incentivize greater resiliency for infant formula supply, encourage new entrants into the market, and diversify the supply chain, without adversely impacting programmatic costs and the number of infants served by the WIC contract models.
While infant formulas – and particularly specialty and metabolic formulas – are regulated by FDA as food, they are in many ways comparable to life-saving medications. Viewing these products through the lens of how FDA addresses drug shortage monitoring and mitigation supports the need for a more responsive mechanism to monitor for and mitigate against potential supply chain disruptions. FDA’s foods regulatory program has and can continue to benefit from the expertise and experience available within the Agency’s medical product centers in this regard. The importance of a team with clinical, nutritional, and analytical expertise cannot be emphasized too much.
Strengthening data and technology tools at FDA and other agencies is also critical to enhancing infant formula supply chain resiliency. The industry has sophisticated supply chain data enabling modeling and predictive analytics for the individual manufacturers and suppliers, but there is no data system to combine the information into a composite picture that would enable an understanding of the resiliency of the entire system to stresses, disruptions, and changes in demand. We need a sustainable mechanism for infant formula supply chain monitoring to allow us to better identify and address existing and future potential supply chain disruptions. A dynamic, interconnected supply chain monitoring platform and robust data sets are necessary to enable the Agency to be most effective in monitoring food supply chains, managing risks, and identifying and quickly addressing supply chain disruptions to reduce impacts on consumers.
One example of a beginning to this effort is FDA’s 21 Forward platform, which has been essential to our infant formula supply chain efforts. Further development of the technology will allow us to integrate, analyze, and monitor multiple data sets – including data on consumer purchasing, in-stock product availability, food facility registration, and imports – in real time to inform our response and help us focus on the areas of greatest need.
In the President’s FY 2023 budget request, we have also identified legislative changes that would provide new tools to help FDA signal our partners who control supply chain dynamics to take action that would prevent or mitigate shortages of infant formula and essential medical foods. Our proposal would require firms to notify FDA of anticipated significant interruptions in the supply of infant formula or essential medical foods, similar to how drug manufacturers do today. These notifications would allow the Agency to receive relatively imprecise – but helpful – indicators about likely or confirmed shortages in the U.S. marketplace, better enabling us to alert the system and stimulate the industry and government partners to take steps that promote the continued availability of these important foods, which often are a sole source of nutrition.
Another component of this proposal would be requiring manufacturers to develop and implement risk management plans. These are routine in most industries and have been used in our drug shortages supply chain oversight. These plans would identify, evaluate, and manage risks to the supply of infant formula or essential medical food. These plans would serve supply chain resiliency within each manufacturer, but they would also be available to FDA for its real-time monitoring efforts of the way they fit together to produce a complete picture of resiliency and vulnerability of this vital supply chain.
None of these improvements would be as useful as a digital platform that monitors the supply chain constantly and in real time. This industry and most others have been resistant to efforts to develop such a system, but until such steps are taken, the American public will be vulnerable to threats from natural disasters and cyberattacks as well as the quality problem that created the current infant formula situation.
Another legislative change identified in the President’s FY 2023 budget request is access to records in lieu of or in advance of an inspection, or, in other words, the authority to conduct remote regulatory assessments. Presently, FDA has such authority for drug inspections, and the Agency often relies on voluntary participation for remote regulatory assessments of many non-drug establishments. However, reliance on voluntary requests is not sufficient to achieve effective and efficient oversight, as firms can refuse to provide records or other information in advance of or in lieu of an inspection or to participate in remote regulatory assessments. We are seeking to expand the explicit statutory authority in section 704(a)(4) of the Federal Food, Drug, and Cosmetic Act to require firms to provide records or other information pertaining to all FDA-regulated products. An expansion across the board, in advance of or in lieu of inspections, would significantly enhance FDA’s ability to obtain access remotely to records and other information from facilities producing infant formulas and essential medical foods, and would help the Agency investigate emerging supply chain issues, promote regulatory compliance, and protect the public health.
Conclusion
Ensuring the availability of safe, sole-source nutrition products like infant formula is of the utmost importance to FDA. Our teams have been working tirelessly with all the responsible entities across government to address and alleviate supply issues while protecting safety, and we will continue doing everything within our authority to ensure the production of safe infant formula products.
Thank you, and we look forward to answering any questions you may have.
__________________
The White House, Building Resilient Supply Chains, Revitalizing American Manufacturing, and Fostering Broad- based Growth: 100-day Reviews under Executive Order 14017, June 2021, available at https://www.whitehouse.gov/wp-content/uploads/2021/06/100-day-supply-chain-review-report.pdf.
U.S. Food and Drug Administration, “Form 483: Inspectional Observations; Abbott Nutrition, Sturgis, Michigan Facility,” September 20-24, 2021, available at https://www.fda.gov/media/156747/download?utm_medium=email&utm_source=govdelivery.
See full testimony for appendix – FDA Testimony ECOI Infant Formula 5.25.2022 final
I know a bit about hearings:
 My email and phone have been a bit busy this weekend with people reaching out who have received notice of the Jif peanut butter recall. Some have opened and unopened jars, some are presently ill or they and family have been sick over the last several weeks. Most have suffered without seeking medical treatment, and those that have received treatment have not received a stool culture to determine if the illness is caused by Salmonella, specifically, Salmonella Senftenberg.
My email and phone have been a bit busy this weekend with people reaching out who have received notice of the Jif peanut butter recall. Some have opened and unopened jars, some are presently ill or they and family have been sick over the last several weeks. Most have suffered without seeking medical treatment, and those that have received treatment have not received a stool culture to determine if the illness is caused by Salmonella, specifically, Salmonella Senftenberg.
Late Friday as I boarded a plane from New Orleans to Seattle, the FDA announced that it and the CDC’s review of epidemiological information indicated that five out of five people reported consuming peanut butter and four of the five people specifically reported consuming different varieties of Jif brand peanut butter prior to becoming ill with Salmonella Senftenberg. There has been a recall in both the United States and Canada thus far.
Interestingly, the FDA also reported that it had conducted (presumably recently) Whole Genome Sequencing (WGS) analysis on an environmental sample collected at the Lexington, KY, J.M. Smucker Company facility in 2010 and found Salmonella Senftenberg.
Total Illnesses of Salmonella Senftenberg that are a WGS match to each other and the 2010 environmental sample, thus far are 14 with 2 hospitalizations in the following states: Arkansas (1), Georgia (2), Illinois (1), Massachusetts (1), Missouri (1), Ohio (1), North Carolina (1), New York (1), South Carolina (1), Texas (2), Virginia (1), and Washington (1). Last Illness Onset: May 1, 2022.
Interesting fact, according to the CDC, for every one person who is a stool-culture confirmed positive victim of Salmonella in the United States, there is a multiple of 38.5 who are also sick, but remain uncounted. (See, AC Voetsch, “FoodNet estimate of the burden of illness caused by nontyphoidal Salmonella infections in the United States,” Clinical Infectious Diseases 2004; 38 (Suppl 3): S127-34).
Friday night the FDA, along with CDC and state and local partners, reported that they are investigating a multistate outbreak of Salmonella Senftenberg infections linked to certain Jif peanut butter products produced at the J.M. Smucker Company facility in Lexington, Kentucky.
Total Illnesses: 14, Hospitalizations: 2, Last Illness Onset: May 1, 2022. States with Cases: Arkansas (1), Georgia (2), Illinois (1), Massachusetts (1), Missouri (1), Ohio (1), North Carolina (1), New York (1), South Carolina (1), Texas (2), Virginia (1), and Washington (1).
CDC’s review of epidemiological information indicates that five out of five people reported consuming peanut butter and four of the five people specifically reported consuming different varieties of Jif brand peanut butter prior to becoming ill. FDA conducted Whole Genome Sequencing (WGS) analysis on an environmental sample collected at the Lexington, KY, J.M. Smucker Company facility in 2010.
The analysis shows that this 2010 environmental sample matches the strain causing illnesses in this current outbreak. Epidemiologic evidence indicates that Jif brand peanut butter produced in the J.M. Smucker Company facility located in Lexington, KY, is the likely cause of illnesses in this outbreak. J.M. Smucker Company has voluntarily recalled certain Jif brand peanut butter products that have the lot code numbers between 1274425 – 2140425 manufactured in Lexington, KY.
It reminded me of another Salmonella outbreak. Beginning in November 2008, CDC PulseNet staff noted a small and highly dispersed, multistate cluster of Salmonella Typhimurium isolates. The outbreak consisted of two pulsed field gel electrophoresis (PFGE) defined clusters of illness. The first cluster displayed a unique primary enzyme (XbaI) restriction pattern and an uncommon secondary enzyme (BlnI) pattern. The second cluster had two closely related XbaI patterns that were very similar to the first cluster and a BlnI pattern that was indistinguishable from the first cluster. Illnesses continued to be revealed through April 2009, when the last CDC report on the outbreak was published. A total of 714 were sickened, with 171 hospitalized and at least nine deaths.
Peanut butter and peanut butter containing products produced by the Peanut Corporation of America plant in Blakely, Georgia, were implicated. King Nut brand peanut butter was sold to institutional settings. Peanut paste was sold to many food companies for use as an ingredient. Implicated peanut products were sold widely throughout the USA, 23 countries and non-U.S. territories.
So, what have we learned? Not, enough!
 Following the tragedy of the PCA Salmonella peanut outbreak in 2008-2009, that sickened over 700 and killed nine, Dr. Stephen Sundlof of the Food and Drug Administration told lawmakers that agency inspectors will start to routinely collect samples for bacterial testing whenever they go into a peanut butter manufacturing facility.
Following the tragedy of the PCA Salmonella peanut outbreak in 2008-2009, that sickened over 700 and killed nine, Dr. Stephen Sundlof of the Food and Drug Administration told lawmakers that agency inspectors will start to routinely collect samples for bacterial testing whenever they go into a peanut butter manufacturing facility.
“We are changing that now as a result of this (outbreak),” Sundlof, head of the FDA’s food safety center, told the House Energy and Commerce investigations subcommittee. The panel is looking for ways to prevent another outbreak like the one that has sickened some 600 people and is being linked to nine deaths. More than 1,900 products have been recalled.
Peanut butter may also be singled out for special attention. Sundlof said the government is weighing whether to designate it as a high-risk food. That means producers would be required to follow written food safety plans to prevent contamination.
Also in 2009, the US Food and Drug Administration (FDA) issued two sets of recommendations for reducing the risk of Salmonella contamination in peanut products, one aimed at the food industry and the other at food service establishments and retail stores.
The FDA’s action follows a 2-month investigation of a nationwide Salmonella Typhimurium outbreak linked to peanut butter, peanut paste, and other items made by Peanut Corporation of America (PCA) that has sickened 683 people in 46 states and has led to the recall of more than 2,833 products. The FDA published the documents on its Web site.
In its guidance for the food industry, the FDA said the document isn’t a set of guidelines, but rather its current thinking on addressing the risk of Salmonella contamination in foods that contain peanut products. It pointed out that Salmonella can become heat resistant as the water activity of a food becomes lower, conditions found in peanut butter and peanut paste.
The effectiveness of processing methods to reduce Salmonella in food products may depend on if and how much an ingredient with low water activity is rehydrated. Processing methods are more effective at killing the pathogen when the peanut ingredient is completely mixed into a high–water activity food, given time to fully rehydrate, and heated or acidified adequately. However, the pathogen may remain when lumps or swirls of peanut butter remain in the food product.
The FDA recommends that food manufacturers obtain peanut products only from suppliers that have validated procedures to reduce Salmonella contamination.
In instances when manufacturers must use raw shelled or blanched peanuts or when Salmonella concerns have been raised about a particular lot or lots of peanut ingredients, the FDA recommends that manufacturers:
Following the passage of the Food Safety Modernization Act (FSMA) in 2011, the FSMA requires FDA to designate high-risk foods for which the proposed additional recordkeeping requirements “are appropriate and necessary to protect the known safety risks of a particular food, including the history and severity of the public health.” The high-risk food designation must be based on the following factors:
Did that ever happen?
Tonight the FDA, along with CDC and state and local partners, are investigating a multistate outbreak of Salmonella Senftenberg infections linked to certain Jif peanut butter products produced at the J.M. Smucker Company facility in Lexington, Kentucky. Total Illnesses: 14, Hospitalizations: 2, Last Illness Onset: May 1, 2022. States with Cases: Arkansas (1), Georgia (2), Illinois (1), Massachusetts (1), Missouri (1), Ohio (1), North Carolina (1), New York (1), South Carolina (1), Texas (2), Virginia (1), and Washington (1). CDC’s review of epidemiological information indicates that five out of five people reported consuming peanut butter and four of the five people specifically reported consuming different varieties of Jif brand peanut butter prior to becoming ill. FDA conducted Whole Genome Sequencing (WGS) analysis on an environmental sample collected at the Lexington, KY, J.M. Smucker Company facility in 2010. The analysis shows that this 2010 environmental sample matches the strain causing illnesses in this current outbreak. Epidemiologic evidence indicates that Jif brand peanut butter produced in the J.M. Smucker Company facility located in Lexington, KY, is the likely cause of illnesses in this outbreak. J.M. Smucker Company has voluntarily recalled certain Jif brand peanut butter products that have the lot code numbers between 1274425 – 2140425 manufactured in Lexington, KY.
I bit(e), or spread, of history:
In 1996, 15 people were sickened after eating peanut butter that was contaminated with S enterica serovar Mbandaka, according to a 1998 report published in the Australia and New Zealand Journal of Public Health. Investigators traced the contamination source to roasted peanuts.
In November 2006, public health officials detected a substantial increase in reports of Salmonella Tennessee isolates. In February 2007, a multistate, case-control study linked the consumption of either Peter Pan or Great Value Peanut Butter brands with infection. 715 people were sickened with 129 hospitalized. Subsequently the same strain of Salmonella Tennessee was isolated from unopened jars of peanut butter and from environmental samples collected from the processing plant. The product was recalled, and new illness reports declined. Unsanitary conditions at the Sylvester, Georgia, processing plant were known about since 2004. On April 5, 2007, ConAgra announced inadvertent moisture from a leaking roof and sprinkler system could have promoted bacteria growth in the plant. Great Value brand was sold at Walmart stores.
Beginning in November 2008, CDC PulseNet staff noted a small and highly dispersed, multistate cluster of Salmonella Typhimurium isolates. The outbreak consisted of two pulsed field gel electrophoresis (PFGE) defined clusters of illness. The first cluster displayed a unique primary enzyme (XbaI) restriction pattern and an uncommon secondary enzyme (BlnI) pattern. The second cluster had two closely related XbaI patterns that were very similar to the first cluster and a BlnI pattern that was indistinguishable from the first cluster. Illnesses continued to be revealed through April 2009, when the last CDC report on the outbreak was published. A total of 714 were sickened, with 171 hospitalized and at least nine deaths. Peanut butter and peanut butter containing products produced by the Peanut Corporation of America plant in Blakely, Georgia, were implicated. King Nut brand peanut butter was sold to institutional settings. Peanut paste was sold to many food companies for use as an ingredient. Implicated peanut products were sold widely throughout the USA, 23 countries and non-U.S. territories.
On September 22, 2012, the CDC announced a multistate outbreak of Salmonella serotype Bredeney linked to Trader Joe’s Valencia Creamy Salted Peanut Butter. Collaborative efforts by local, state and federal public health and regulatory officials traced the product to Sunland, Inc. a Portales, New Mexico company. Sunland issued a recall of multiple nut butters and products made with nut butters. When the outbreak was declared over, a total of 42 people infected with the outbreak strain of Salmonella serotype Bredeney had been reported by 20 states. Among persons for whom information was available, illness onset dates ranged from June 14, 2012 to September 21, 2012. Ill persons ranged in age from less than 1 year to 79 years, with a median age of 7 years. Sixty-one percent of ill persons were children less than 10 years old. Among 36 persons with available information, 10(28%) patients had been hospitalized. The FDA confirmed that environmental samples collected at the Sunland facility had an DNA fingerprint that was indistinguishable to the DNA fingerprint found in outbreak associated patients.
On August 21, 2014, the CDC announced a multistate outbreak of Salmonella Braenderup involving 6 people residing in Connecticut (1), Iowa (1), New Mexico (1), Tennessee (1), and Texas (2). Almond and peanut butter manufactured by nSpired Natural Foods, Inc. was named as the likely source of this outbreak. The outbreak was declared over on October 16, 2014. Illness onset dates range from January 22, 2014 to May 16, 2014. Among 5 ill persons with available information, one person reported being hospitalized. During inspections at the nSpired Natural Food facility in Ashland, Oregon, between January 2014 and August 2014, the FDA isolated Salmonella Braenderup from environmental samples. A search of the PulseNet database linked ill patients to the environmental isolates taken from the nSpired production plant. On August 19, 2014 nSpired Natural Foods issued a voluntary recall of certain lots of almond and peanut butters because of potential contamination with Salmonella. The recalled brands include Arrowhead Mills, MaraNatha, and specific private label almond and peanut butters.
On December 2, 2015 JEM Raw Chocolate LLC (JEM Raw) of Bend, Oregon announced a recall of its full line of all nut butter spreads due to possible contamination with Salmonella. Health authorities at the FDA, Oregon Health Authority, Oregon Department of Agriculture and the CDC had linked illnesses in 13 persons who consumed nut spreads. Dates of onset ranged from July 18, 2015 to November 22, 2015. Cases were reported from California, Colorado, Georgia, Hawaii, Idaho, Illinois, Maine, North Carolina, New Jersey and Oregon.
In March 2017, the Centers for Disease Control and Prevention (CDC) and several state health departments attributed a multistate outbreak of Shiga toxin-producing Escherichia coli O157:H7 to I.M. Healthy brand SoyNut Butter manufactured by Dixie Dew and sold at retail on online outlets. Outbreak investigators collected open containers of SoyNut Butter from the homes of sick people, and unopened containers from retail locations. Containers of SoyNut Butter from lots #243162 and 244161 tested positive for E. coli. Whole genome sequencing revealed that the same strain of E. coli was found in clinical isolates from sick people and containers of I.M. Healthy SoyNut Butter. Epidemiologic investigation determined that 32 people ill with this strain of E. coli had been infected by eating or attending a facility that served I.M. Healthy SoyNut Butter. This included residents of Arizona (4), California (5), Florida (2), Illinois (1), Massachusetts (1), Maryland (1), Missouri (1), New Jersey (1), Oregon (11), Virginia (2), Washington (2), and Wisconsin (1).
References:
https://pubmed.ncbi.nlm.nih.gov/9744205/
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5621a1.htm
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm58e0129a1.htm
https://www.cdc.gov/salmonella/bredeney-09-12/
https://www.cdc.gov/salmonella/braenderup-08-14/
In 30 years of practice, I have on numerous occasions offered to FDA leadership the opportunity to meet directly with the people who consumed food that was tainted under the FDA’s watch. I have always thought that if they only had the chance to meet the victims and their families, they would understand just how important their jobs really are. Regardless of administration, I have yet to have a taker.

Lucas Parker, 2-year-old Canadian boy with possible pre-existing autism spectrum disorder exposed to Romaine lettuce contaminated with E. coli O157:H7 on a family road trip to Disneyland from British Columbia.
Onset of pain and bloody diarrhea on 10/18/18 causing family to head home. Made it as far as Olympia, WA ER where Lucas presented with bloody diarrhea, vomiting, nausea, and pain, diagnosed as a gastrointestinal infection and dehydration. Continued their way home but condition deteriorated the following day with Lucas becoming only minimally responsive with high fever, high blood pressure, increasing diarrhea, and dehydration. Admitted to B.C. hospital. When his kidneys began to fail and his lab work showed red blood cell destruction, he was diagnosed with HUS. Transferred to tertiary care children’s hospital on 10/21/18.
Developed seizure activity with severe decline in his neurological functioning and started on anti-convulsant medication. Intubated for head imaging and surgery. Catheter surgically inserted in abdomen for peritoneal dialysis. On 10/25 Shiga toxin 2 confirmed in the lab. More seizures on 10/28 despite medication. Labile blood pressures increased white cell count, and recurrent high blood sugars concerning for sepsis. Remained on mechanical ventilation. More seizure activity on 10/28 worrisome for brain injury with ongoing kidney failure and hemolysis (red blood cell destruction).
Kidney function began to return after 13 days but prognosis was poor given evidence of worsening brain damage. Extubated on 16th hospital day but still on dialysis for fluid removal. At high risk for aspiration due to lack of consistent gag/cough reflex. Surgery on 11/16 to remove peritoneal dialysis catheter and implant a feeding tube. Transferred to rehab facility on 11/18 bedbound in fixed, supine position, with limited visual and neurological function.
Went into respiratory distress after inadvertent drug overdose and readmitted to hospital were treated for complications of HUS including stroke, severe neurological deficit, dystonia and autonomic dysregulation (slow heart rate, high blood pressure, irregular breathing). Head imaging confirmed further brain damage. Experienced intermittent drops in his oxygen saturation levels with possible additional seizure activity and apnea (episodes of cessation of breathing). By 12/03 he was intermittently hypotensive and experiencing recurrent vomiting.
Condition stabilized and returned to rehab on 12/11/18 for multidisciplinary therapy to try to maximize function. He was assessed at a “near coma” level of consciousness with severe cognitive impairment and severe cortical visual impairment. Unable to sit, stand or maintain his head/neck/trunk position independently, with spasticity in his arms and legs, consistent with quadriplegia. He had no meaningful vocalizations and was receiving nutrition through a feeding tube.
Prognosis includes ESRD (end stage renal disease), diabetes, lifelong monitoring of his renal status, multiple kidney transplants, and prolonged periods of dialysis. Neurological deficits unlike to improve over lifetime and is at risk for hip dislocation and scoliosis due to spasticity.
Medical Bills……………………………………………$593,230.38
In 30 years of practice, I have on numerous occasions offered to FDA leadership the opportunity to meet directly with the people who consumed food that was tainted under the FDA’s watch. I have always thought that if they only had the chance to meet the victims and their families, they would understand just how important their jobs really are. Regardless of administration, I have yet to have a taker.
Sandra Antle, 75-year-old married, very active mother and grandmother, with remote history of chronic lymphocytic leukemia, otherwise in very good health before falling ill.
Onset of fatigue and diarrhea on 09/06/11, progressing over next several days, leading to ER visit on 09/09. Tentative diagnosis was a urinary tract infection and enteric infection with C. diff. She was admitted and started on antibiotics. The following day blood cultures confirmed Listeria and antibiotic coverage was expanded. She went into respiratory distress with high blood pressure and she was rushed to the ICU where she was intubated for mechanical ventilation. A central catheter was placed in her neck for medication and blood draws.
She developed pulmonary edema (fluid in the lungs) and signs of heart failure. The bacteria was confirmed in her bloodstream, including her spinal fluid and brain. Brain imaging confirmed fluid buildup, resulting in extreme somnolence and unresponsiveness. On 09/13 surgery was performed to drill a hole in her skull to drain off some of the fluid that was putting pressure on her brain.
She continued to deteriorate, however, and remained intubated and increasingly unresponsive. On 09/18 the family, after consultation with Sandy’s doctors whose advised that she was showing no indication of any brain activity and her prognosis—a vegetative state—was bleak, decided to disconnect life support. Sandy died on 09/18, just more than one week after first becoming sick.
Medical Bills……………………………………………$200,810.15
Craig Baldwin, 65-year-old widower and aeronautical engineer, with two adult children, on autoimmune medication for a history of pemphigus (an autoimmune dermatological condition), otherwise in good health before becoming infected.
Onset of fatigue and tremulousness on 09/07/11, increasing over the next two weeks to include total body fatigue and dyscoordination, leading to an ER visit on 09/22. No diagnosis was made and Craig was sent home, where he rapidly deteriorated. Admitted to the hospital the following day at which time brain and neck imaging showed multiple lesions. Craig became acutely weak and disoriented with slurred speech. His mental function began to decline with short term memory loss, speech disorder, right facial droop, and right sided weakness. Diagnostic workup continued and he was started on antibiotics for empiric infection.
On 9/24 the lab confirmed Listeria and antibiotic therapy was adjusted. Craig’s condition worsened with loss of right sided function. Brain imaging showed new bleeding in the brain consistent with abscesses from Listeria. Surgery was performed to obtain a biopsy of brain tissue which resulted positive for Listeria. There were signs of acute kidney injury. With antibiotic therapy, his brain infection and cognitive function began to improve.
After 29 days in the hospital, Craig was transferred to the rehab unit on 10/07 for intensive therapy to restore strength and conditioning. He was evaluated for his persistent cognitive deficits and attendant anxiety and depression about his physical and mental deficits. After 1 and ½ months of therapy, he was discharged home on 11/15 with need for full time assistance in mobility, activities of daily living, and cognitive and emotional support, along with regular outpatient therapy. He received daily speech, physical and occupational therapy through the end of 01/12. He was left with permanent physical and cognitive deficits.
Medical Bills……………………………………………$607,379.46
Will Burkes, Sr., 72-year-old married man employed as a mechanic’s assistant who was receiving chemotherapy for colorectal cancer when he became infected.
Symptoms began on 09/07/11 with high fever, severe headache, confusion, and slurred speech. He was admitted to the ICU for evaluation and management with antibiotics for probably bacterial meningitis. He was intubated for mechanical ventilation for airway protection and respiratory failure. On 09/09 labs resulted positive for Listeria and antibiotics were adjusted.
Testing indicated acute heart attack and rhythm changes. He developed atrial fibrillation (ineffective heartbeat that can lead to blood clots) and further workup confirmed impaired heart function and probable congestive heart failure. Diuretics were prescribed to try to relieve some of the fluid buildup in Will’s lungs. Will was able to be extubated on 09/13. He was put on medication for high blood pressure.
Will underwent cardiac catheterization on 09/16 to assess the patency of his coronary arteries and the function of the left side of his heart. He began to show signs of stabilization despite ongoing diarrhea and pulmonary insufficiency.
On 9/21 Will underwent abdominal surgery because of concern that a portion of his colon was ischemic (lacking sufficient blood supply) but surgical findings were negative and the impression was pneumatosis (gas within the wall of the intestine). During this entire time, Will was unable to eat because of high risk of aspiration, and was getting nutrition through a feeding tube. He completed antibiotic therapy which seemed to have successfully treated his infection. He was discharged to a skilled nursing facility on 10/6 after one month in the hospital.
At the nursing facility, he worked with physical, occupational and speech therapy to restore his strength and stamina and was gradually advanced from tube to oral feedings. He was discharged after six weeks of care. He continued to be treated on an outpatient basis for gastrointestinal issues, dizziness, word finding difficulty, and slurred speech, and he remained at risk of aspiration due to ongoing difficulties with swallowing.
Medical Bills……………………………………………$407,287.22
George Drinkwater, 81-year-old married, retired school board member and school bus driver with four adult sons, eight grandchildren, and 14 great grandchildren. Prior medical history of myelodysplastic syndrome (pre-leukemia), coronary artery disease, orthopedic issues, and gastrointestinal bleeding, all under control by his physicians. https://vimeo.com/71609746
Symptoms came on in the middle of the night on 09/09/11. He collapsed when trying to get out of bed and began vomiting uncontrollably. He became incontinent of bowel and bladder during the ambulance ride to the ER. In the ER he was found to have a fever and was diagnosed with pneumonia and gastroenteritis and admitted for treatment. His fever continued, despite medication, along with severe headaches and diarrhea. By 09/12 he began vomiting again and his condition deteriorated significantly.
George was transferred by airlift to a higher level tertiary care facility on 09/13. His heart was in atrial fibrillation (ineffective rhythm creating risk of blood clot), and he became incoherent with no control over his extremities, all consistent with sepsis (inflammatory response to overwhelming infection) and encephalitis (brain inflammation). Brain imaging was negative and a spinal fluid sample was obtained. He stopped breathing and a code team responded to resuscitate him. The family decided, after discussion with his care team, that George would not want to be intubated or undergo CPR in the event of another arrest and a DNR (do not resuscitate) order was put in place.
His course continued to deteriorate, and he died on 09/14, after five days in the hospital.
Medical Bills……………………………………………$103,316.16
Rene Gaxiola, 63-year-old married Apostolic Church bishop and church pastor with one son, suffering from terminal brain cancer in home hospice care at the time he became infected.
Symptoms began on the morning of 09/07/11 with fever and unresponsiveness. The hospice nurse arrived and found his fever to be very high with elevated blood pressure. Medics were called and by the time they arrived, Rene was only semi-conscious, his heart rate was rapid, and he was unable to speak.
Rene was transported to the ER and found to be “essentially unresponsive” by neurological examination. His temperature was over 106°F. While workup was taking place to try to determine the etiology of his symptoms, Rene was started on antibiotics and admitted. Given his underlying terminal cancer diagnosis, DNR status, and progressively deteriorating condition, however, Rene’s family and caregivers decided to transfer him to inpatient hospice for comfort care only.
Rene continued to decline at hospice and on 09/10 he was noted to be “actively dying.” He died on the evening of 09/10, after three days in the hospital.
Medical Bills……………………………………………$23,105.35
William Pumphery, 84-year-old married father and grandfather, retired from a career in the Air Force, with a history of chronic lymphocytic leukemia, and coronary artery disease in stable condition before he became ill.
Symptoms began in early 09/11 with lethargy, weakness, mental status changes, and loss of balance leading to three falls. He became acutely ill on 09/07 with fever, shaking, jerking and unresponsiveness. He was rushed to the ER where he was admitted with fever and weakness, and started on empiric antibiotics. Over the next couple of days, he showed signs of improvement but on 09/10 his blood cultures resulted positive for Listeria, indicative of septicemia (blood poisoning by bacteria). He developed acute on chronic kidney insufficiency. Bill’s mental status changes were concerning for meningoencephalitis (inflammation of the brain) and he had generalized bruising all over his extremities.
While Bill was improved enough by 09/13 to transfer out of the ICU to transitional care, on 09/15 he became more confused and weaker, and was unable to even lift himself out of a chair. His wife, despite being advised by his doctors that he would not likely survive a code, declined to change his status to DNR (do not resuscitate). Over the next week, labs confirmed that he was in progressive kidney failure and by 09/20 his doctors decided to start him on dialysis. By 09/22, Bill was barely oriented to his surroundings and his kidneys were producing no urine at all.
Bill’s blood pressure began to fall and he was bleeding around his catheter insertion site. He received blood products to try to stabilize him hemodynamically, but it was clear that his condition was dire and his prognosis was poor. His wife asked that he be kept alive until their children could arrive from out of the country to say goodbye. On 09/24, Bill was intubated for mechanical ventilation and put on multiple medications to try to raise his blood pressure. Later that day, the family agreed to comfort care measures only, and Bill died that afternoon. He spent 17 days in the hospital.
Medical Bills……………………………………………$102,851.21
John Riffle, 95-year-old married, former Army intelligence officer, farmer and cattle breeder. When he became infected, John was on dialysis for end stage renal disease and he had heart and lung issues. He was mentally intact, however, and completely independent in his daily activities.
John’s symptoms came on in late September 2011. He was seen in the ER on 09/30 for shortness of breath and he was medicated for a presumed urinary tract infection. At a doctor’s visit on 10/11 John was found to have fluid in one of his lungs, thought to be from the infection in his urinary tract. The following day, however, he became weaker and shorter of breath, and he returned to the ER, where blood cultures resulted positive for Listeria. John was admitted for treatment of rapid heartbeat and low blood pressure, consistent with sepsis (inflammatory response to overwhelming infection). With initiation of IV antibiotics, John made some initial improvement, despite development of a painful, itchy rash on his back.
On 10/25, the day John was to be discharged home, he went into respiratory distress. Chest x-rays confirmed pneumonia. Dialysis continued for John’s failing kidneys and to try to relieve some of the fluid buildup in his lungs. On 10/31, after 20 days in the hospital, John’s condition suddenly deteriorated. He became progressively unresponsive and he died on 11/1.
Medical Bills……………………………………………$10,335.62
Paul Schwartz, 92-year-old former life insurance agent, married father of five, grandfather of nine, and great grandfather of ten. Paul had pre-existing age-related medical conditions including high blood pressure, heart disease, degenerative joint disease, and glaucoma but was active and independent. Before falling ill, he was also the primary caregiver for his wife who was suffering from Alzheimer’s disease.
Paul began to feel weak, especially in his legs, on 09/13/11 followed by confusion and loss of appetite. He was seen in the ER on 09/16 but no diagnosis was made. After he returned home, he began to experience increasing abdominal pain and mental status changes, and returned to the hospital where he was admitted for treatment of acute kidney injury attributed to a viral infection. On 09/22 blood cultures confirmed Listeria. He was treated with antibiotics for sepsis (inflammatory response to overwhelming infection) and meningoencephalitis (inflammation of the brain). Over the next several weeks, his medical condition began to stabilize, but he became more agitated and delirious, remaining mostly non-communicative. Given his disorientation and confusion, he was unable to participate in therapy to restore his strength and conditioning.
After five weeks in the hospital, on 10/21 Paul was discharged to a skilled nursing facility. He continued to decline, with hypoxic respiratory distress and atrial fibrillation (irregular heartbeat which can result in blood clots). He fell on 11/04, developed a bladder infection, and required full assistance for all activities of daily life. He was given supplemental oxygen to compensate for his respiratory distress. His mental status continued to deteriorate, he became agitated at times, and was found several times in a kneeling/praying position on the floor next to his bed. He was too confused and disoriented to be able to participate in therapy.
On 12/18 he was again found on the floor, but this time he was completely unresponsive with no detectable blood pressure or oxygen saturation. He was taking only three breaths per minute. The family decided that they did not want him transferred back to the hospital and comfort measure were provided. Paul died later that day.
Medical Bills……………………………………………$181,384.65
Chris Wallace, 51-year-old fabric business owner with prior history of rheumatoid arthritis on immunosuppressants, and high blood pressure, who was otherwise independent and active before becoming ill.
Chris first began experiencing symptoms in early September 2011 with nausea, vomiting, diarrhea, and fever. On 09/07 he became very confused and disoriented with worsening gastrointestinal symptoms. His partner took him to the ER, where he was started on empiric antibiotics and admitted for presumed meningitis/encephalitis (inflammation of the brain). While waiting for the results of lab studies, his doctors suspected a possible stroke. Chris was so confused he pulled out his lines and catheter, so his wrists were tied to his bed frame. His fever gradually subsided and his condition stabilized, his confusion seemed better, but he was markedly weak. All of his blood cultures had been negative.
On 09/15 he was transferred to an inpatient rehab facility for therapy. Within a few days, Chris was rushed back to the hospital for falling blood pressure, increased short term memory loss, and lethargy. More blood and spinal fluid were drawn for testing. Brain imaging studies showed increased lesions, inconsistent with stroke or bleeding. Antibiotic coverage was adjusted, given widespread news of a community outbreak of Listeria, but still without lab confirmation in Chris’s case, likely attributable to the fact that he had been receiving antimicrobial therapy when the specimens were obtained. Chris was treated for an enteric infection with C. diff.
Although Chris remained stable during this hospitalization. He was discharged to home on 10/3 on outpatient penicillin infusion for six weeks and orders to follow up with multiple specialists. After discharge, Chris continued to struggle with the effects of permanent brain injury and memory loss, and was dependent upon his partner for all of his daily needs.
Medical Bills……………………………………………$269,189.44
Clarence Wells, 87-year-old widower and former Pentagon lithographer, with two children, four grandchildren, and two great grandchildren, independent in most all of his daily living activities, residing with his daughter and her family.
Clarence became ill in late August 2011. He was seen in the ER on 08/25 in critical condition with a history of bloody stools for several days, swelling, and signs of poor blood perfusion. He was transferred by ambulance to a tertiary care ICU with diagnoses of congestive heart failure, respiratory distress, kidney insufficiency, anemia, electrolyte imbalances, and risk for bleeding. After several days of treatment in the ICU, his condition seemed to stabilize, and he began therapy to try to restore some of his strength and conditioning.
Clarence’s condition took a turn for the worse on 08/31 with a rapid heartbeat, fever, difficulty breathing, and mental status changes, consistent with sepsis (inflammatory response to overwhelming infection). He was confused with a slight facial droop. By the early evening, his pulse was undetectable, and his pupils were dilated and non-reactive to light. After six days in the hospital, he passed away that night.
Medical Bills……………………………………………$30,381.99
Florence Wilcox, 96-year-old widow with two sons and eight grandchildren, generally in good health with age-related medical issues including high blood pressure, acid reflux, and bladder issues. She lived independently and actively before becoming ill.
Florence’s symptoms began in early September 2011. On 09/08 Florence was having bloody diarrhea, was weak and dehydrated, and she was running a fever. She called for an ambulance and medics rushed her to the ER. At the hospital her temperature was recorded at 104.9°F, she was started on empiric antibiotics, with a diagnosis of sepsis (inflammatory reaction to overwhelming infection). Her condition worsened and she became unresponsive. She was airlifted to a tertiary care facility for specialty care.
Florence was admitted to the ICU with diagnoses of encephalopathy (brain swelling), sepsis, and altered mental status. Concern arose that she had suffered a stroke because of absent reflexes in her arms and legs. Her heart was in atrial fibrillation (irregular heartbeat concerning for clots). Imaging showed fluid buildup in her lungs and she was having difficulty breathing. By 09/11 she was completely unresponsive. A feeding tube was inserted into her esophagus to maintain nutrition. A spinal fluid sample was drawn for analysis which tested positive for Listeria.
Over the next few days, EEG testing revealed general cerebral slowing with possible epilepsy and Florence was started on prophylactic antiepileptic medication. Doctors advised Florence’s son that his mother was dying and, given her advanced age and the extent of her brain injury, any attempts to resuscitate her would likely be followed by further deterioration and more medical emergencies that would ultimately take her life. After one week in the hospital, on 09/15 she suffered a systolic arrest and she died.
Medical Bills……………………………………………$180,248.54
 According to the CDC and FDA, at least 4 kids were sickened and of those two died, from drinking Abbott infant formula. Abbott denies the connection. However, the resulting investigation and inspection (and whistleblower documents) uncovered enough problems in the Abbott facility to shutter it causing havoc with supplies of infant formula. The facility is now set to reopen, but not before the U.S. Attorney sued Abbott and several employees. In the complaint, filed by the U.S. Department of Justice on behalf of the FDA, the government alleges that powdered infant formula products manufactured at Abbott Nutrition’s Sturgis facility were adulterated because they were made under insanitary conditions and in violation of current good manufacturing practice requirements.
According to the CDC and FDA, at least 4 kids were sickened and of those two died, from drinking Abbott infant formula. Abbott denies the connection. However, the resulting investigation and inspection (and whistleblower documents) uncovered enough problems in the Abbott facility to shutter it causing havoc with supplies of infant formula. The facility is now set to reopen, but not before the U.S. Attorney sued Abbott and several employees. In the complaint, filed by the U.S. Department of Justice on behalf of the FDA, the government alleges that powdered infant formula products manufactured at Abbott Nutrition’s Sturgis facility were adulterated because they were made under insanitary conditions and in violation of current good manufacturing practice requirements.
Abbott is essentially confessing to the violations in the below consent decree. Under the proposed consent decree, Abbott Nutrition will be required to retain an independent expert to review the Sturgis facility’s operations to ensure compliance with the law. It also includes requirements for testing products, as well as ceasing production, and promptly notifying the FDA should contamination be detected. The proposed consent decree also requires the implementation of a sanitation plan, environmental monitoring plan and employee training programs.
Here are the key documents:
Here is the 2021 inspection report at the plant – APPLIED – FOI II – BR Abbott Nutritions- FEI# 1815692 9-2021 EIR.
Here are the whistleblower documents – Redacted Confidential Disclosure re Abbott Laboratories – 10-19-2021_Redacted (1)
Here is the 2022 inspection report at the plant – Updated Final Applied_Unapplied Redactions Abbott Nutrition Sturgis FEI 1815692 FDA 483 1-31022 to 3-16-22 – ISSUED_Redacted
Here is the complaint – abbott_complaint_0
Here is the consent decree – abbott_proposed_consent_decree_0
Please read the above and ask the question: is this how infant formula should have been manufactured?
So, what gives the government the right to charge a company and certain employees with either a felony or a misdemeanor?
Congress passed the Federal Food, Drug, and Cosmetic Act in 1938 in reaction to growing public safety demands. The primary goal of the Act was to protect the health and safety of the public by preventing deleterious, adulterated or misbranded articles from entering interstate commerce. Under section 402(a)(4) of the Act, a food product is deemed “adulterated” if the food was “prepared, packed, or held under insanitary conditions whereby it may have become contaminated with filth, or whereby it may have been rendered injurious to health.” A food product is also considered “adulterated” if it bears or contains any poisonous or deleterious substance, which may render it injurious to health. The 1938 Act, and the recently signed Food Safety Modernization Act, stand today as the primary means by which the federal government enforces food safety standards.
Chapter III of the Act addresses prohibited acts, subjecting violators to both civil and criminal liability. Provisions for criminal sanctions are clear:
Felony violations include adulterating or misbranding a food, drug, or device, and putting an adulterated or misbranded food, drug, or device into interstate commerce. Any person who commits a prohibited act violates the FDCA. A person committing a prohibited act “with the intent to defraud or mislead” is guilty of a felony punishable by years in jail and millions in fines or both.
A misdemeanor conviction under the FDCA, unlike a felony conviction, does not require proof of fraudulent intent, or even of knowing or willful conduct. Rather, a person may be convicted if he or she held a position of responsibility or authority in a firm such that the person could have prevented the violation. Convictions under the misdemeanor provisions are punishable by not more than one year or fined not more than $250,000, or both.
The legal jargon aside, if you are a producer of food and knowingly or not manufacturer and sell adulterated food, you can (and should) face fines and jail time.