In twenty-four days, the same company has turned up at the center of two separate federal foodborne illness investigations. One is the largest Cyclospora outbreak this country has ever recorded. The other is a Salmonella Javiana outbreak that has sickened 345 people in 27 states. That does not happen to most produce companies in a decade. It has happened to Taylor Farms in a month, and the two are not the same kind of problem. I represent people sickened in these outbreaks and in several of the older ones below. That is a disclosure.
Start with the lettuce. FDA’s advisory, last updated August 5, counts 6,358 illnesses in fifteen states, at least 278 hospitalizations and two deaths in Michigan, with onsets from June 22 through July 31. CDC’s outbreak page carries the same figures. Those are laboratory-confirmed cases tied to Taco Bell or the recalled lettuce. My own fifty-state chart, built from what the states publish about themselves, stood at 27,937 cases across thirty-eight states last night. Maine became the sixteenth outbreak state on Friday, in a formal advisory from its own health department, and the federal count still says fifteen.
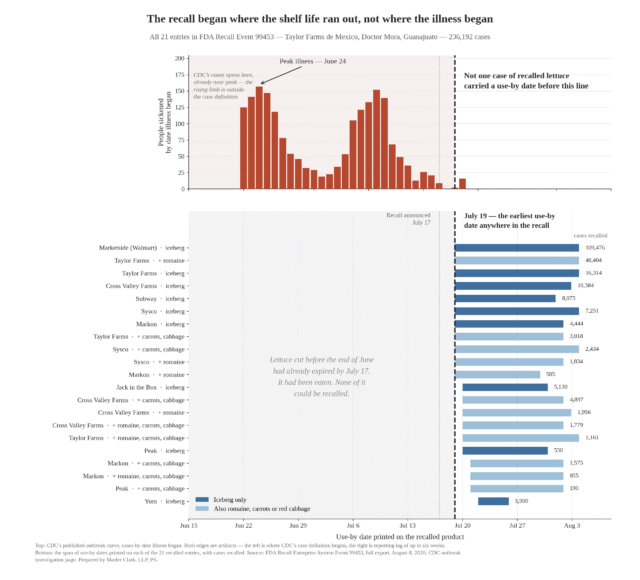
The recall behind it was announced July 17 by Taylor Farms de Mexico, out of the Doctor Mora plant in Guanajuato. FDA’s own enforcement file runs to twenty-one entries and 236,192 cases of lettuce, sold to nine customers including Subway, Sysco, US Foods and Walmart’s Marketside label.
Now the peppers, and here I am going to be fair before I am critical. Taylor Farms did not grow these jalapeños. A grower in Sinaloa did. Coast Citrus Distributors of San Diego imported them and sold them to wholesalers, restaurants and processors. FDA’s traceback converged on that grower, FDA recommended that Coast Citrus recall, and Taylor Fresh Foods recalled its own finished products on August 9 after its supplier notified it. On the jalapeños, Taylor Farms is a buyer handed a contaminated ingredient, the same as Chipotle and Kroger, and anyone reading a list of recalled salsa should understand that first.
What is worth writing about is the scale. Twenty products came off the shelf, into Hannaford, Kroger, Stop and Shop, Target, Trader Joe’s, Walmart and Whole Foods, and into distribution centers in twenty-six states. USDA issued a separate public health alert the day before for meat and poultry made with the same peppers, most of it out of Taylor Farms plants. One grower in Sinaloa, one importer in San Diego, and within a weekend the list reaches seven of the largest grocery banners in the country.
Count the products on that list with Taylor Farms on the package. There are five, all at Target. The other fifteen are Private Selection, Freshness Guaranteed, Trader Joe’s, or carry no brand at all. A shopper holding a tub of Kroger Spicy Pimento Cheese Dip has no way of knowing who made it. That is the private label business working as designed, and it is why telling people to check the refrigerator is not a plan.
And FDA still has not named the Sinaloa grower. It named Coast Citrus. Its advisory names Chipotle and QDOBA, and CDC’s investigation page counts twenty-seven illness clusters at those chains. The grower whose peppers are the reason for all of it stays confidential, while in the Cyclospora advisory FDA put Taco Bell in the first sentence and Taylor Farms de Mexico in the headline. I cannot find the principle that produces both results.
Anna Skinner at Newsweek published a timeline of Taylor Farms recalls and outbreaks on Monday that goes back seventeen years, and she deserves credit for how she did it. She built it partly off a review I put together, then did the harder half of the job. She called the company and printed its answer in full. She printed the entries Taylor Farms disputes and said so plainly.
Four days earlier CNN published an investigation of its own, by Casey Tolan, Yahya Abou-Ghazala, Curt Devine and Kyung Lah, arguing that this outbreak follows a years-long pattern of deflected blame. The key finding came from a former senior FDA food official, who told CNN that the 2024 McDonald’s onion investigation was a slam dunk and that Taylor Farms went to considerable lengths to keep the agency from naming it publicly. It did not work that time. Nobody had to make that argument about the 2024 romaine outbreak, because no agency named anyone at all.
CNN also put numbers on the oversight. FDA has not inspected the Guanajuato plant since 2019, and in the first half of this year five of the company’s more than 160,000 Mexican shipments were physically examined. Taylor Farms’ Mexican subsidiaries are the largest source of vegetable and salad shipments into this country of any manufacturer in the world.
In 2013 Bruce Taylor said the tests were negative and there was no evidence of Cyclospora in the product. In 2015, after a Montana laboratory found E. coli in the celery and onion mix behind the Costco outbreak, the one that put two children into kidney failure, he told the Monterey Herald it looked like a false alarm. In 2024 the company said its testing found no traces in the onions, in an outbreak that killed a man in Colorado. In 2026 it went to a false positive on a single border sample. Four outbreaks, one answer: the testing was clean. It is clean because people eat the evidence. A negative result on what is left in the cooler is not a finding of innocence.
The Newsweek timeline repeats that FDA apologized over the false positive. That apology is the company’s own characterization, from its July 19 statement. FDA’s record contains a laboratory correction and no apology; CNN reports the agency denied apologizing, and the company took its social media post down. In the same update FDA said it was continuing to work with the firm to remove product implicated in the outbreak. The word implicated survived the retraction.
Here is the company’s position, stated fairly. Taylor Farms says it invests more than $200 million a year in food safety, that it acted voluntarily and more broadly than asked on the lettuce, and that it put traceback protocols in place ahead of the Food Traceability Rule deadline. Take that last claim at face value and two questions have documented answers in its own files. How many days passed between the first Sinaloa pepper entering a Taylor Farms plant and the recall list being published, and how many between FDA’s first call about iceberg lettuce and the July 17 removal? A company with real time traceability can answer both in an afternoon.
What I want out of August is short. FDA should classify the July 17 lettuce recall, which three weeks on is still marked Not Yet Classified and has therefore never appeared in a weekly enforcement report. FDA should name the Sinaloa grower. Recall notices should carry customer names rather than brand codes, so buyers two steps down the chain know what is in their walk-in. And Taylor Farms should produce the water testing records and the adjacent land reviews for the Doctor Mora ranches, because its own website says both exist.