
Clostridium botulinum is an obligate anaerobic, spore-forming, Gram-positive bacillus whose primary, native habitat is the soil.[1] The bacterium that thrives in low-oxygen environments and produces botulinum neurotoxin, one of the most lethal biological substances known. While the bacteria themselves are usually harmless, the toxin they create attacks the nervous system and causes botulism, a severe paralytic illness.
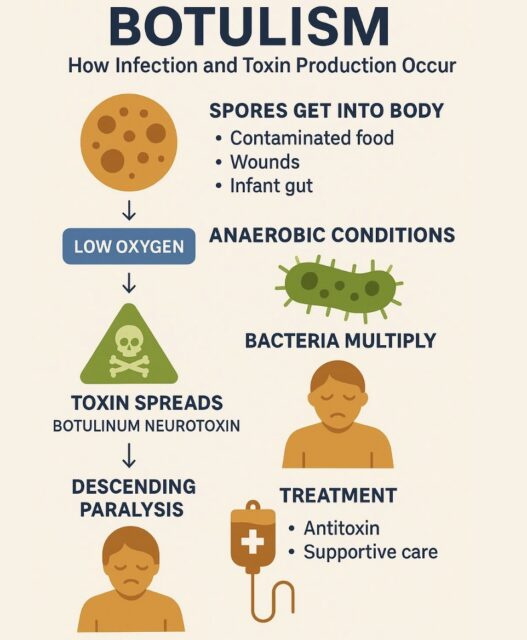
Types of Botulism:
- Foodborne: Caused by eating foods contaminated with the toxin, often from improper home-canning or poorly preserved foods.
- Infant: Occurs when babies (under one year old) ingest the bacterial spores, which then germinate and produce toxins in the gut. This is why honey should never be fed to infants.
- Wound: Happens when C. botulinum spores infect a cut or wound and produce toxins, commonly associated with the use of contaminated injection drugs.
- Iatrogenic Botulism: A rare type that occurs if too much botulinum toxin is injected for cosmetic purposes (like wrinkle reduction) or medical conditions (like migraines
- Adult Intestinal Toxemia: An extremely rare condition in older children and adults where spores colonize the intestinal tract and produce toxin (similar to infant botulism)
Where Does Clostridium botulinum Come From?
- Soil and Sediment: The Ultimate Natural Reservoir
Landmark environmental surveys dating back over a century have established that viable C. botulinum spores reside in ground soils, dust, and aquatic sediments across every continent where they have been sought. The distribution of specific toxin types in infant botulism cases typically reflects the geographic prevalence of those strains in the local soil. For example, in the United States, Type A spores are predominantly found in the western states, while Type B spores are more densely concentrated in the eastern and mid-Atlantic states.

- Airborne Dust and Environmental Displacement
Because spores are highly resistant to environmental stressors (such as drying, heat, and UV light), they easily become airborne. Presently, dust inhalation or ingestion is considered a primary, unavoidable exposure route.[2] (Dabritz et al., 2025). Epidemiological data significantly associates infant botulism cases with residence in windy or dusty locations, as well as proximity to dust-generating activities.
- Honey: The Primary Identifiable and Avoidable Food Source
While environmental exposure is largely unpreventable, honey is universally recognized as the single most significant, avoidable foodborne vehicle for C. botulinum spores.[3] (Arnon et al., 1979; Harris & Dabritz, 2024). C. botulinum is not a disease of the honeybee. Instead, honey becomes an accidental repository when bees carry environmental dust, water, or pollen contaminated with spores back to the hive.[4] (Schneider et al., 2004). Because honey is typically consumed raw (unpasteurized and non-irradiated), and because bacterial spores are uniquely structurally adapted to survive low-moisture environments, the dormant spores remain viable inside the honey matrix indefinitely. Globally, about 4% of retail honey specimens test positive for Clostridium botulinum spores, though regional rates vary widely. While some localized surveys find no spores, others report contamination rates as high as 10% to 20% depending on the source and processing methods. [5]
- Infant Botulism and Clostridium botulinum
Infant botulism is a rare but serious paralytic illness of babies, usually affecting infants younger than one year. It is caused when an infant swallows spores of Clostridium botulinum, or rarely related toxin-producing Clostridium species, and those spores survive, germinate, and multiply in the immature intestine. The bacteria then produce botulinum neurotoxin inside the infant’s gut. In plain terms, the baby does not simply ingest a “germ”; the infant’s bowel becomes the place where the toxin is made.[6] [7]
That mechanism is what separates infant botulism from classic foodborne botulism. In foodborne botulism, a child or adult typically swallows toxin that has already formed in contaminated food. In infant botulism, the infant swallows spores, and the toxin is produced after the spores colonize the intestine. Infants are uniquely vulnerable because their gut microbiome, bile-acid profile, immune defenses, and intestinal motility are still developing, and they do not yet have the mature protective intestinal flora that usually prevent C. botulinum spores from gaining a foothold in older children and adults.[8] [9] Approximately 95% of cases occur in infants under six months of age, with a median age of around three months. Most cases are caused by toxin type A or type B.[10] Because they are so common, in many individual cases the exact source is never identified.[11]
- Signs and Symptoms in Infants
Infant botulism often begins subtly and then progresses over hours to days. Constipation is commonly one of the earliest signs, followed by poor feeding, weak suck, weak or altered cry, drooping eyelids, diminished facial expression, reduced gag reflex, poor head control, generalized hypotonia, lethargy, and respiratory difficulty. CDC’s clinical overview specifically lists constipation, poor feeding, ptosis, sluggish pupils, flattened facial expression, diminished suck and gag reflexes, weak or altered cry, and respiratory difficulty or arrest as typical findings.[12] Common signs include:
- Constipation, often for several days;
- Poor feeding, with weak sucking and swallowing;
- A weak, altered, or soft cry;
- Drooping eyelids (ptosis), sluggish pupils, and reduced eye movement;
- Generalized weakness and low muscle tone—the classic “floppy baby”;
- Lethargy and a diminished gag reflex; and
- Breathing difficulty, progressing in severe cases to respiratory failure—the most dangerous complication.
Because these early signs mimic more common conditions, a high index of suspicion matters. A baby with poor feeding, a weak cry, and increasing floppiness—especially with any breathing difficulty—needs urgent evaluation.[13]
- Botulism in Older Children and Adults
The same toxin can cause serious illness in older children and adults, but the exposure pattern is different. Foodborne botulism occurs when a person eats food in which toxin has already formed, classically improperly canned, preserved, fermented, or stored low-acid foods. Wound botulism occurs when spores contaminate a wound and produce toxin in devitalized tissue; in modern U.S. practice, this is often associated with injection-drug use. Iatrogenic botulism can occur after excessive or improperly administered therapeutic or cosmetic botulinum toxin. Adult intestinal colonization botulism is rare but can occur when the adult gut is altered by surgery, antibiotics, bowel disease, or other disruptions.[14] [15]
In non-infant botulism, symptoms often begin with cranial nerve findings such as blurred or double vision, drooping eyelids, slurred speech, difficulty swallowing, dry mouth, and facial weakness. Weakness then typically descends symmetrically from the face and neck to the arms, trunk, and legs. Patients are usually awake and afebrile, and sensation is usually preserved, which can make the paralysis especially frightening. Severe cases require intubation and mechanical ventilation. Id.
- Diagnosis and Laboratory Detection
Botulism is first and foremost a clinical diagnosis. Laboratory confirmation is important, but treatment should not wait for test results when the clinical picture is concerning. CDC’s 2021 clinical guidelines emphasize that timely diagnosis is crucial because antitoxin is the only specific therapy and should be administered as quickly as possible.Because the antitoxin works best when given early, clinicians treat as soon as infant botulism is reasonably suspected.[16]
For infants, definitive testing usually requires stool or enema specimens, which can be tested for botulinum toxin and cultured for C. botulinum. Testing is specialized and is generally coordinated through state public health laboratories, CDC, and the California Department of Public Health Infant Botulism Treatment and Prevention Program. CDC advises that this specialized testing often takes days and that clinicians should not delay BabyBIG treatment while awaiting confirmation. [17]
In outbreak investigations, public health laboratories may also test leftover foods, unopened products, ingredients, environmental samples, and bacterial isolates from patients. Whole-genome sequencing can compare isolates from patients, products, and ingredients to determine whether they are genetically related. In the ByHeart outbreak, that genetic comparison was central because isolates from clinical samples, finished formula, base mix, and organic whole milk powder clustered together.[18] [19]
- Treatment
Infant botulism is highly treatable, and the great majority of babies recover fully. Care rests on two pillars: specific antitoxin and supportive care.[20] Treatment has two parts: neutralizing circulating toxin and supporting the patient while nerves recover. For infants, the specific treatment is human botulism immune globulin intravenous, known as BIG-IV or BabyBIG. BabyBIG is FDA-approved for infant botulism types A and B and is obtained in the United States through the Infant Botulism Treatment and Prevention Program. The treating physician contacts the program for immediate consultation; if the presentation supports infant botulism, BabyBIG is released and treatment begins without waiting for final laboratory confirmation. [21] [22]
The evidence for BabyBIG is strong. In a randomized, double-blind, placebo-controlled California trial of 122 infants with laboratory-confirmed infant botulism, treatment within three days of hospital admission reduced mean hospital stay from 5.7 weeks to 2.6 weeks. It also reduced ICU time, mechanical ventilation time, tube or intravenous feeding time, and hospital charges. In plain language, BabyBIG does not instantly make the baby well, but it stops additional circulating toxin from binding and can substantially shorten the illness.[23]
Supportive care is equally important. Infants may need close ICU monitoring, respiratory support, mechanical ventilation, suctioning, prevention of aspiration, nutritional support through nasogastric or other tube feeding, bowel care, occupational therapy, feeding therapy, physical therapy, and careful discharge planning. Antibiotics are generally not used to treat infant botulism itself because bacterial killing in the gut may increase toxin release; aminoglycosides and certain other medications that impair neuromuscular transmission are avoided because they can worsen weakness.[24]
For older children and adults with suspected foodborne, wound, or other non-infant botulism, the specific antitoxin is generally heptavalent botulinum antitoxin, obtained through public health authorities and CDC. As with infants, antitoxin should be given as early as possible, because it neutralizes toxin that has not yet bound to nerves. Wound botulism also requires wound evaluation and debridement, and antibiotics may be used for wound infection after antitoxin decisions are addressed. [25] [26]
- Prognosis, Recovery, and Complications
With prompt recognition, BabyBIG, and modern intensive care, most infants survive and recover. The favorable survival statistics, however, should not minimize the seriousness of the acute illness. That favorable long-term prognosis, however, should not obscure the severity of the acute illness, which is frightening, often protracted, and frequently requires weeks of intensive hospital care. The recognized complications include:
- Respiratory failure, apnea, and aspiration—the principal reason a ventilator may be required (on average roughly three weeks when needed);
- Prolonged feeding difficulty—safe oral feeding can take many weeks to return;
- Autonomic effects such as urinary retention, and secondary infections (e.g., pneumonia, ear infection) acquired in the hospital;
- Prolonged general weakness during recovery. [27] [28] [29]
A baby with infant botulism may spend days to weeks unable to feed safely, protect the airway, or breathe without support. Families may experience a prolonged hospitalization, transfer to a tertiary children’s hospital, repeated testing, feeding-tube dependence, ventilator care, and months of follow-up. [30] In the 2025 ByHeart-formula outbreak, CDC EIS preliminary data found that approximately two-thirds of evaluated infants required post-hospitalization physical therapy or feeding support.”[31] Reasonable follow-up commonly includes primary care, neurology as needed, feeding or speech therapy, physical and occupational therapy, nutrition monitoring, developmental surveillance, and assessment for residual weakness, dysphagia, oral aversion, motor delay, or caregiver trauma. Id. Lasting neurological after-effects are seldom seen, and most infants regain normal strength and development; severe long-term harm is rare. Follow-up with neurology and physiotherapy is advisable after a severe episode.[32]
[1] Jin, J. (2023). What is botulism?. Journal of the American Medical Association (JAMA), 330(1), 90-90. https://jamanetwork.com/journals/jama/issue/330/1
[2] Dabritz, H. A., Chung, C. H., Read, J. S., & Khouri, J. M. (2025). Global occurrence of infant botulism: 2007–2021. Pediatrics, 155(4), e2024068791.
[3] Harris, R. A., & Dabritz, H. A. (2024). Infant botulism: in search of Clostridium botulinum spores. Current Microbiology, 81(10), 306. https://link.springer.com/article/10.1007/s00284-024-03828-0
[4] Schneider, K. R., Schneider, R. M. G., Kurdmongkoltham, P., & Bertoldi, B. (2025). Preventing foodborne illness: Clostridium botulinum. https://ask.ifas.ufl.edu/publication/FS104
[5] Harris, R. A., & Dabritz, H. A. (2024). Infant botulism: in search of Clostridium botulinum spores. Current Microbiology, 81(10), 306. https://link.springer.com/article/10.1007/s00284-024-03828-0
[6] CDC. Clinical Overview of Infant Botulism. April 24, 2024. https://www.cdc.gov/botulism/hcp/clinical-overview/infant-botulism.html
[7] Rao AK, Sobel J, Chatham-Stephens K, Luquez C. (2021). Clinical Guidelines for Diagnosis and Treatment of Botulism. MMWR Recomm Rep. 2021;70(2):1-30. https://www.cdc.gov/mmwr/volumes/70/rr/rr7002a1.htm
[8] CDC. Clinical Overview of Infant Botulism. April 24, 2024. https://www.cdc.gov/botulism/hcp/clinical-overview/infant-botulism.html
[9] Rosow LK, Strober JB. Infant Botulism: Review and Clinical Update. Pediatr Neurol. 2015;52(5):487-492. PubMed/PMC access: https://pmc.ncbi.nlm.nih.gov/articles/PMC10332751/
[10]American Academy of Pediatrics, supra note 3; CDC, National Botulism Surveillance Summary, 2021, https://www.cdc.gov/botulism/php/national-botulism-surveillance/2021.html.
[11]American Academy of Pediatrics, supra note 3; American Family Physician (AAFP), Infant Botulism, https://www.aafp.org/pubs/afp/issues/2002/0401/p1388.html.
[12] CDC. Clinical Overview of Infant Botulism. April 24, 2024. https://www.cdc.gov/botulism/hcp/clinical-overview/infant-botulism.html
[13] Children’s Hospital Los Angeles, supra note 2; Merck Manual, supra note 1.
[14] Rao AK, Sobel J, Chatham-Stephens K, Luquez C. Clinical Guidelines for Diagnosis and Treatment of Botulism, 2021. MMWR Recomm Rep. 2021;70(2):1-30. https://www.cdc.gov/mmwr/volumes/70/rr/rr7002a1.htm
[15] Jeffery IA, Nguyen AD, Karim S. Botulism. [Updated 2024 Nov 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459273/
[16] Rao AK, Sobel J, Chatham-Stephens K, Luquez C. Clinical Guidelines for Diagnosis and Treatment of Botulism, 2021. MMWR Recomm Rep. 2021;70(2):1-30. https://www.cdc.gov/mmwr/volumes/70/rr/rr7002a1.htm
[17] CDC. Clinical Overview of Infant Botulism. April 24, 2024. https://www.cdc.gov/botulism/hcp/clinical-overview/infant-botulism.html
[18] CDC. Investigation Update: Infant Botulism Outbreak, November 2025. March 4, 2026. https://www.cdc.gov/botulism/outbreaks-investigations/infant-formula-nov-2025/investigation.html
[19] FDA. Outbreak Investigation of Infant Botulism: Infant Formula (November 2025). Content current as of June 3, 2026. https://www.fda.gov/food/outbreaks-foodborne-illness/outbreak-investigation-infant-botulism-infant-formula-november-2025
[20] Jeffery IA, Nguyen AD, Karim S. Botulism. [Updated 2024 Nov 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459273/
[21] CDC. Clinical Overview of Infant Botulism. April 24, 2024. https://www.cdc.gov/botulism/hcp/clinical-overview/infant-botulism.html
[22] Scarborough, A. P., Khouri, J. M., Chung, C. H., Dabritz, H. A., & Read, J. S. (2025). International Experience with Human Botulism Immune Globulin for the Treatment of Infant Botulism. Medical Research Archives, 13(10). https://esmed.org/MRA/mra/article/view/7026
[23] Scarborough, A. P., Khouri, J. M., Chung, C. H., Dabritz, H. A., & Read, J. S. (2025). International Experience with Human Botulism Immune Globulin for the Treatment of Infant Botulism. Medical Research Archives, 13(10). https://esmed.org/MRA/mra/article/view/7026
[24] Rao AK, Sobel J, Chatham-Stephens K, Luquez C. Clinical Guidelines for Diagnosis and Treatment of Botulism, 2021. MMWR Recomm Rep. 2021;70(2):1-30. https://www.cdc.gov/mmwr/volumes/70/rr/rr7002a1.htm
[25] Jeffery IA, Nguyen AD, Karim S. Botulism. [Updated 2024 Nov 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459273/
[26] Scarborough, A. P., Khouri, J. M., Chung, C. H., Dabritz, H. A., & Read, J. S. (2025). International Experience with Human Botulism Immune Globulin for the Treatment of Infant Botulism. Medical Research Archives, 13(10). https://esmed.org/MRA/mra/article/view/7026
[27] Scarborough, A. P., Khouri, J. M., Chung, C. H., Dabritz, H. A., & Read, J. S. (2025). International Experience with Human Botulism Immune Globulin for the Treatment of Infant Botulism. Medical Research Archives, 13(10). https://esmed.org/MRA/mra/article/view/7026
[28] Morris, V., Wians, R., Wilson, J., & Stevens, G. (2022). Infant Botulism. Journal of Education & Teaching in Emergency Medicine, 7(2), S48. https://pmc.ncbi.nlm.nih.gov/articles/PMC10332751/
[29]Public Health Agency of Canada, supra note 6.
[30] Scarborough, A. P., Khouri, J. M., Chung, C. H., Dabritz, H. A., & Read, J. S. (2025). International Experience with Human Botulism Immune Globulin for the Treatment of Infant Botulism. Medical Research Archives, 13(10). https://esmed.org/MRA/mra/article/view/7026
[31] CDC EIS Conference. Severity of Illness and Clinical Outcomes of Infants Linked to an Infant Botulism Outbreak Caused by Powdered Infant Formula — United States, 2025. April 17, 2026. https://www.cdc.gov/eis-conference/php/abstracts/infant-botulism-outbreak-caused-by-powdered-infant-formula.html
[32] AAFP, supra note 5; Public Health Agency of Canada, supra note 6; Botulism Sequelae: A Systematic Review, PMC, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12798721/.