
Here is the link to the website – https://www.fda.gov/food/outbreaks-foodborne-illness/investigations-foodborne-illness-outbreaks
Here is the link to the website – https://www.fda.gov/food/outbreaks-foodborne-illness/investigations-foodborne-illness-outbreaks
DATE AND TIME November 3, 2022, from 10:00 A.M. to 4:00 P.M. ET
The Food Safety and Inspection Service (FSIS) is considering a regulatory framework for a new strategy to control Salmonella in raw poultry products and more effectively reduce foodborne Salmonella infections linked to these products. This framework identifies the key elements that the Agency is currently considering as part of a new regulatory strategy. FSIS is soliciting feedback from stakeholders, both at a public meeting and in written comments submitted to the meeting docket in the Federal Register, on all of the elements of the framework before moving forward with any proposed changes to regulations or other actions.
View the Proposed Regulatory Framework to Reduce Salmonella Illnesses Attributable to Poultry
FSIS is interested in your feedback on the three components as well as the cross-cutting issues described within the framework. Specifically, we would appreciate comments and input on the following questions:
FSIS also welcomes relevant scientific evidence or examples of how these components may be implemented or the impacts they may have on human Salmonella illnesses.
The meeting will be virtual and will be viewed via the Zoom link provided by email when you register for the meeting. Attendees must pre-register for the meeting.
Stakeholders who wish to speak at the public meeting must notify FSIS during registration and must register by October 24, 2022. Oral comments will be limited to two minutes per component. Attendees must identify which component(s) (i.e. the 3 components and cross-cutting issues) they will be commenting on when they register for the public meeting. FSIS will do its best to accommodate all persons who pre-registered and requested to provide oral comments. FSIS will notify stakeholders that register to speak of the approximate time(s) they are scheduled to speak in advance of the meeting.
Attendees that do not plan to speak at the public meeting may register at any time up to the day of the meeting. Interested persons will have 30 days to comment after the meeting notice is published in the Federal Register. Submit comments via Regulations.gov.
Additional details are available in Docket No. FSIS-2022-0029.
Borrowing a bit from Dylan.
We shall see if this new move from FSIS is more aspirational or more realistic.
However, despite not have any clear time lines or regulations, things I never thought I would hear from the USDA/FSIS:
23% of foodborne Salmonella illnesses are attributable to poultry consumption.
… Considering requiring … incoming flocks be tested for Salmonella.
FSIS is assessing whether certain levels or types of Salmonella on raw poultry product present an elevated risk of causing human illness such that they should be considered adulterants. As a result, the Agency is considering implementing a final product standard or standards to ensure that product contaminated with Salmonella that is likely to make people sick is not sold to consumers.
I am reminded of Voltaire’s quote: “The perfect is the enemy of the good.”
I still think my Salmonella Petition would be perfect – https://www.regulations.gov/document/FSIS-2020-0007-0001
But as Otto von Bismarck said: “Politics is the art of the possible.”
Here is the full release at 3:15 AM:















Mary Kay Billman
Mrs. Billman ate ice cream at the 3350 Bahia Vista in Sarasota, Florida location on January 2022, and died of a Listeria infection on January 29, 2022. She left a husband, children and grandchildren.
Mrs. Billman fell ill on or around January 27, 2022, with symptoms consistent with Listeria. Mrs. Billman was admitted to Memorial Regional Hospital South on January 27, 2022, where a stool sample was collected that day and tested positive for Listeria serotype ST5. Mrs. Billman ultimately passed away on January 29, 2022. Medical bills were $89,689.02.
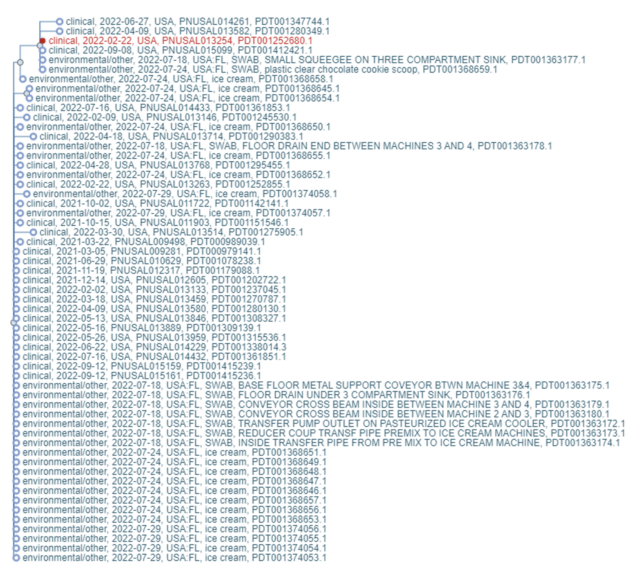
Further testing of this specimen at the Florida Department of Health confirmed that her Listeria had the allele code LMO1.1 – 43.2.2.85.126.1 and was associated with the “multistate cluster” given the CDC code 2110MLGX6-4. This was ultimately the Listeria outbreak associated with Big Olaf’s ice cream. Ice cream was also closely genetically matched to Mrs. Billman’s isolate.
As of June 29, 2022, a total of 23 people infected with the outbreak strain of Listeria monocytogenes have been reported from 10 states. Of the 22 people with information, 20 sick people reported living in or traveling to Florida in the month before they got sick, although the significance of this is still under investigation. Illnesses started on dates ranging from January 24, 2021, through June 12, 2022.
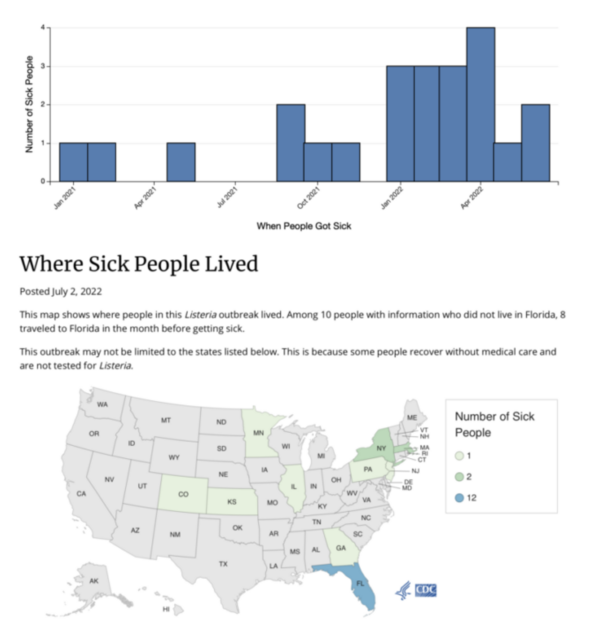
The Florida Department of Health, CDC, public health and regulatory officials in several other states, and the U.S. Food and Drug Administration (FDA) are collecting different types of data to investigate a multistate outbreak of Listeria monocytogenes infections. As a result of this investigation, Big Olaf Creamery in Sarasota, FL, is voluntarily contacting retail locations to recommend against selling their ice cream products. Consumers who have Big Olaf Creamery brand ice cream at home should throw away any remaining product.
Public health officials continue to interview people about the foods they ate in the month before they got sick. Of the 17 people interviewed, 14 (82%) reported eating ice cream. Among 13 people who remembered details about the type of ice cream they ate, six reported eating Big Olaf Creamery brand ice cream or eating ice cream at locations that might have been supplied by Big Olaf Creamery.
On July 1, 2022, Big Olaf Creamery in Sarasota, FL, voluntarily began contacting retail locations to recommend against selling their ice cream products. Consumers who have Big Olaf Creamery brand ice cream at home should throw away any remaining product.
Public health officials continue to interview people about the foods they ate in the month before they got sick. Of the 17 people interviewed, 14 (82%) reported eating ice cream. Among 13 people who remembered details about the type of ice cream they ate, six reported eating Big Olaf Creamery brand ice cream or eating ice cream at locations that might have been supplied by Big Olaf Creamery.
Listeria has been found on equipment in the ice cream processing facility and in 16 of 17 flavors. Big Olaf first refused to recognize that it was the cause of the outbreak and refused to stop production and stop ice cream sales. According to the Florida Department of Agriculture and Consumer Services (FDACS):
“The results from product sampling taken from the Big Olaf production facility last week by FDACS found that 16 of the 17 flavors tested were positive for Listeria monocytogenes (L. mono). This includes Blueberry Cheesecake, Butter Pecan, Cherry Cordial, Chocolate, Chocolate Chip, Coconut, Coconut Almond Joy, Cookie Dough, Cookies & Cream, Kahlua Krunch, Mint Chip, Pistachio, Plantation Praline, Superman, Vanilla, and White Chocolate Raspberry. With these results, FDACS is currently issuing formal stop sales on the 16 products where L. mono was found, which were previously part of a voluntary recall. Our department continues to work closely with our state and federal partners on this investigation and enforcement of the stop sale.”
Please find linked here the results for the product samples that represent the 16 positive flavors. The one outstanding environmental sample noted previously has also come back positive, bringing the total positive environmental samples to 10, and I’m linking here those results.

The Tennessee Department of Health recently released a report from last Summer’s tragic E. coli O157:H7 Outbreak linked to goat contact. I sadly need to update www.fair-safety.com. Full disclosure, we are representing two families.
Background
On Wednesday, June 22, the Tennessee Department of Health (TDH) was notified of an ill child hospitalized in Florida with Shiga Toxin-Producing E. coli (STEC) O157:H7 after attending a goat husbandry summer camp at a local farm in Rutherford County, Tennessee. The TDH received a second call on Saturday, June 25 from the same mother stating she knew of a 2-year-old patient hospitalized at Vanderbilt in Nashville, TN with hemolytic uremic syndrome (HUS) and reported that this child’s older brother had attended the same camp. The Foodborne and Enteric Diseases (FED) Program staff searched Vanderbilt Medical Center’s electronic medical records confirming the child had STEC and was admitted for HUS. On the morning of Monday June 27, the FED team initiated an outbreak investigation.
The farm hosting the summer camp, “Farm X,” included many attractions for families such as a petting zoo, pony rides, splash pad, walking trails, various fields and three food service establishments. During the summer months, Farm X held multiple five-day summer camps teaching animal husbandry for children ages 6-10. Among other activities, children pick out a baby goat and care for it the remainder of the camp. Children attended camp during the day and return home each afternoon. Three of these camps took place in 2022 prior to the TDH investigation: June 6-10 (Week 1), June 13-17 (Week 2), and June 20-24 (Week 3). Farm X typically hosts three weeks of camp followed by two weeks of no camp.
Methods
Epidemiology
A list of 82 Summer Camp participants from weeks 1, 2 and 3 and their parent/guardians’ contact information was obtained from Farm X for case finding and exposure assessment. TDH staff sent an online survey to all parents/guardians on Friday, July 1 to provide information about the outbreak and conduct interviews. Questions included symptom profile and duration, illness outcomes, days/weeks of camp attendance, food history specific to lunches and other foods served at the camp, and camp activities. Cases were classified using the following case definitions:
Confirmed Case
o Primary Confirmed Case: A person who attended any of the three Farm X Summer Camps from 6/6/22 – 6/24/22 and tested positive for STEC with a specimen collection date after 6/6/22.
o Secondary Case: A household member or close contact of a Farm X Summer Camp attendee who tested positive for STEC with a specimen collection date after 6/6/22.
Probable Case
o Primary Probable Case: A person who attended Farm X Summer Camp and became ill with diarrhea* within 10 days of attending the Farm X Summer Camp without laboratory confirmation.
o Secondary Probable Case: A household member or close contact of a Farm X Summer Camp attendee that became ill with diarrhea* within 10 days after encountering a primary probable case.
*Diarrhea: Defined as at least 3 or more loose stools within a 24-hour period
Data were collected and stored in RED Cap. The survey was open from Friday, July 1 at 5PM to the afternoon of Friday, July 8. A reminder was sent to camp contacts on Tuesday, July 5 at noon. Odds ratios and Fisher’s exact p-values were calculated to help narrow down different possible exposures of interest on the farm and at the summer camp. If a person did not complete the survey, they were excluded from the analysis.
Environmental Health
On June 28th and 29th, FED and Mid-Cumberland Region Environmental Health staff conducted an environmental assessment (EA) at Farm X. Property owners, management and several staff members were in attendance. The aims of EA activities included an onsite interview and observation, collection of camp attendee registration, goat assignment records, and environmental sampling.
A total of 28 environmental and water samples were collected by the TDH during the site visits (See Appendix II). All samples were delivered to the Tennessee State Public Health Laboratory (SPHL) on the same day of collection. Farm X also collected thirteen goat stool samples, independent of TDH sampling, for testing at Tennessee Department of Agriculture’s C.E. Kord Animal Health Diagnostic Lab (Kord Lab) and water samples for testing at a private laboratory in Nashville named Micobac.
Laboratory
Samples received at the SPHL were tested by polymerase chain reaction (PCR) and if PCR results were positive, isolation of the bacteria was attempted. If isolation was successful, the isolates were sent to the sequencing department for whole genome sequencing (WGS). After initial analysis by the Kord Lab, any specimens where STEC was isolated were sent to the SPHL for WGS. Samples initially tested by the SPHL that were unable to grow STEC were sent to the United States Department of Agriculture (USDA) Agroecosystem Management Research Unit for repeat testing, as this USDA laboratory specializes in animal and environmental STEC testing.
Results
Epidemiology
Eighty-two summer camp attendees were present at Farm X from 6/6/22 – 6/24/22. Fifty-three (65%) surveys were completed using an outbreak-specific questionnaire with twelve cases and fifty-eight controls included in the final analysis.
Twelve primary cases (2 confirmed, 10 probable) and two secondary cases (1 confirmed, 1 probable) were identified. Onset dates ranged from June 10 to June 21, 2022. The epidemiologic curve supports the likelihood most ill primary cases were exposed sometime during the week they attended camp; ten of twelve primary cases attended between June 6 and June 10. The median duration of illness was 4.5 days (Range: 2-20 days). Five cases (36%) were female. The median age among cases was 6 years. Two cases (one primary and one secondary case) went to the ER and were hospitalized. The secondary hospitalized case developed HUS and passed away. Fourteen (100%) cases reported diarrhea, seven (50%) reported stomach cramps, six reported fever (43%), and 5 (36%) reported nausea. The number of new cases peaked on June 13 with three cases stating they began feeling ill on this day.
Campers were served six food options and engaged in seventeen activities (see Appendix I for the full food and activity analysis). When comparing cases with controls (non-ill persons) who attended the camp, none of the food items or activities were statistically significantly associated with illness. Given the camp food and activity schedules were consistent between weeks and most campers ate every food and participated in almost every activity, it is difficult to make meaningful comparisons along these lines. The only statistically significant difference between cases and controls was that cases were more likely to attend camp during week one (OR: 13.1, 95% CI 2.59, 66.57) which is reflected in the epi curve (Figure 2).

Environmental Health
On 6/25/22 Farm X voluntarily closed the facility. During the EA on 6/28/22 the food service aspect of the farm was not operating and general inquiries about food service and preparation were made. No ill food handlers, ill farm staff, or camper illnesses were reported to the farm owners during the three weeks of camp. There were no reports of foodservice system changes during this time and no disruptions in water, sewage, or power were reported. There were no maintenance activities reported for kitchen equipment and the kitchen was in good repair. Farm X owners reported that only pre-cooked food was served to campers and fresh watermelon was offered as an optional selection. Fresh raw, preformed beef burgers were prepared on Thursdays and Fridays and cooked to order but were not offered to campers. FED staff recommended cleaning and sanitizing all food contact surfaces in the kitchen and separating staff duties between farm/animal handlers from food handlers.
There were several handwashing and hand sanitizing stations throughout the facility. The outdoor handwashing stations observed were manually activated by depressing a foot bulb on ground and supplied with cold water (both municipal and chlorinated spring-sourced), soap, and towels. Farm X’s policy requires handwashing immediately following goat handling and prior to food service for campers. For smaller children, Farm X reported that step stools are provided, and staff assists them with pumping the water. Several porta-potty restrooms were provided throughout the facility and are maintained by the staff. Waste contents are removed by third-party, porta-potty vendor. No fecal incidents reported amongst campers during any week of camp.
On 6/28/22 investigators collected twenty environmental samples (See Appendix II Samples # 1-20) and on6/29/22 collected eight water samples (See Appendix II Samples 1.W–8.W). Farm X was able to provide investigators with the camp registration contact list, goat assignment records, lists of daily camp activities, and food service menu calendar. During the onsite visits the farm appeared to be in good repair and the animals seemed well cared for and healthy.
In response to the outbreak, Farm X expedited the already scheduled demolition of the barn housing the baby goats, euthanized two baby goats who had tested positive for STEC, moved the rest of the herd off the property, and indefinitely ceased the animal husbandry aspect of the summer camp. During the closure of the farm, Farm X reportedly consulted with veterinarians from the United States Department of Agriculture (USDA) and the Tennessee Department of Agriculture (TDA). Lastly, to better understand how similar operations address pathogen transmission risk reduction, Farm X reported consulting with other farming operations including visiting three petting zoos.
On 7/18/22 Farm X reopened for summer camp, without the goat husbandry component, and to the public on 7/21/22.
Laboratory
The SPHL received a total 33 environmental samples, eight water samples, and three clinical samples. One clinical specimen was collected in Florida and analyzed for whole genome sequencing by the Florida Department of Health State Laboratory. Of the 33 environmental samples one was a goat feed sample, seventeen were goat stool specimens, and fifteen were environmental swabs. Thirteen of the goat stool specimens were collected independently by the owner of Farm X and were initially analyzed at the Kord Lab. Fifteen of the environmental samples (one goat rectal swab and fourteen goat fecal samples) that initially were unable to grow STEC were sent to the USDA Agro ecosystem Management Research Unit for repeat testing. In total, 45 specimens were collected in response to this outbreak (see Appendix II: Table 2).
Of the 45 samples collected for this outbreak nine were positive for STEC representing three different serotypes: H14 (2 environmental), O157:H7 (3 clinical, 2 environmental), O26 (2 environmental) (See Appendix II: Table 2). One of the H14 specimens was collected by Farm X and initially tested at the KORD laboratory; neither of the H14 or O26 serotypes were associated with clinical illnesses in this outbreak. All five O157:H7 specimens were closely related by WGS. The two environmental samples were from a wooden post inside the barn where the baby goats resided (See Appendix II Sample #12) and from a runny stool (animal origin not confirmed) collected outside on the side of the barn where the baby goats would congregate (See Appendix II: Table 2, Sample #6). Sample 12 was isolated and sequenced by the SPHL and sample 6 was isolated by the USDA’s Agroecosystem Management Research Unit followed by sequencing at the SPHL. All five samples were closely related with a maximum of nine SNPs and average off our SNPs distance between isolates (Figure3). Innermost alleles, which more closely reflect the core genome, four of the five specimens were zero alleles apart (Figure 4). Allele information for the missing specimen is unavailable since it was collected in Florida and the two fecal samples (N22165515-01V and N22165515-01W) were isolates generated from the same specimen (See Appendix II: Table 2, Sample #6).

Discussion & Conclusion
It is well documented that Shiga Toxin-producing E.coli (STEC) resides in the gastrointestinal tract of ruminant animals such as cattle, goats, sheep, deer, and elk without causing illness (Source CDC1). STEC outbreaks have also been well documented specifically in the petting zoo environment both in the United States and globally (Austria 20152, Florida 20073, Virginia 20224, Connecticut 20165, Florida, and Arizona 2004 and 20056).
In June and July of 2022, the TDH investigated an outbreak of STEC E. coli O157:H7 associated with Farm X in Tennessee. Survey responses did not show any statistically significant results in terms of food or camp activity exposures, however attending during the first week of camp (June 6, 2022 – June 10, 2022) was significantly associated with illness. One explanation for this could be that this first week coincided with a period of increased STEC shedding in baby goats, which can happen due to increased stress or environmental changes (Factors Associated with STEC Shedding in Cattle7). Based on the laboratory and epidemiologic findings, this outbreak likely occurred due to close contact with baby goats during their time at the camp. Illness of others who did not attend camp were attributed to secondary exposure to their infected household member. This hypothesis is further strengthened by there being no reports of illness from general admission customers before, during, or after the three weeks of summer camps in question.
During the site visits at Farm X, we reviewed the National Association of State Public Health Veterinarians (NASPHV) Animal Contact Compendium and Resources (NASPHV Animal Contact Compendium8) document. Farm X had awareness of the Compendium and complied with the majority of recommendations potentially limiting additional transmission. Farm X voluntarily closed the farm for three weeks. Upon reopening they removed the baby goat care aspect from camp activities and increased risk communication language on their website and on signage throughout the farm.
STEC is naturally found in the intestinal tracts of healthy ruminant animals like cattle, sheep, and goats (Source CDC1). Proper hand washing is a key control measure to prevent infection with STEC and other harmful germs. The process of vigorously scrubbing the hands with running water and soap helps to remove germs. Use of alcohol-based hand sanitizer can reduce the number of germs on hands but does not replace washing with soap and water (Source CDC9).
TDH recommended they continue to provide an adequate number of accessible hand washing stations (supplied with soap, water, and paper towels), maintain appropriate educational signage throughout the facility, enhance educational messaging on their website, continue to explain this risk on their camp registration forms, and to complete a facility consultation with the University of Tennessee Extension agricultural professionals.
The TDH FED concluded that this outbreak was associated with direct contact with goats infected with STEC O157:H7 with secondary transmission from cases. Control measures in place at the farm to minimize transmission may have reduced additional illnesses and enhanced control measures to reduce risk were recommended.
Here is full Report: https://www.marlerblog.com/files/2022/10/TN22-023-Final-Outbreak-Report_9.29.22.pdf

As of October 7, 2022, 20 people infected with the outbreak strain of E. coli O121 have been reported from 6 states – Michigan, Wisconsin, Iowa, Ohio, Kansas and Florida. Illnesses started on dates ranging from July 13, 2022, to September 13, 2022. Sick people range in age from less than 1 to 71 years, with a median age of 31, and 79% are female. Of 14 people with information available, 5 have been hospitalized, including 1 who developed hemolytic uremic syndrome, a serious condition that can cause kidney failure. No deaths have been reported.
State and local public health officials are interviewing people about the foods they ate in the week before they got sick. Among 18 people interviewed, 15 reported shopping at ALDI stores. Among these 15 ALDI shoppers, 6 reported eating Earth Grown brand frozen falafel purchased from ALDI in the week before getting sick.
Here are some prior E. coli O121 Outbreaks linked to flour, cheese, bison, water, sprouts, mini meals, petting zoos, day care, prison, and a Wendy’s.
Thanks www.outbreakdatabase.com.
Many of the below we have been involved with at Marler Clark.
2021 Multistate Outbreak of E. coli O121 Infections Linked to Cake Batter

Officials in New Zealand investigating Hepatitis A cases linked to berries have identified a connection with a past outbreak in Europe.
There are 12 hepatitis A infections from eating frozen berries in New Zealand. Eight have been linked by genetic sequencing, meaning they were likely exposed to the same source of the virus. Seven people have been hospitalized. The virus attacks the liver. The Ministry for Primary Industries (MPI) was informed by the Ministry of Health of three Hepatitis A cases in September.
Foodstuffs Own Brands has recalled various Pams brand frozen berry products because of a possible link to the hepatitis A cases. Products are being removed from New World, Pak’n Save and Four Square shops nationwide, and from Trents and Raeward Fresh stores in the South Island.
All batches and dates of Pams brand Mixed Berries 500-gram, Two Berry Mix 1-kilogram and 750-gram, Smoothie Berry Mix 500-gram, and raspberries 500-gram and 350-gram are involved.
THE HEPATITIS A VIRUS
Exposure to the hepatitis A virus (“HAV”) can cause an acute infection of the liver that is typically mild and resolves on its own.[1] The symptoms and duration of illness vary a great deal, with many persons showing no symptoms at all.[2] Fever and jaundice are two of the symptoms most commonly associated with HAV infection.[3]
Throughout history, hepatitis infections have plagued humans. The “earliest accounts of contagious jaundice are found in ancient China.”[4] According to the CDC:
The first descriptions of hepatitis (epidemic jaundice) are generally attributed to Hippocrates. Outbreaks of jaundice, probably hepatitis A, were reported in the 17th and 18th centuries, particularly in association with military campaigns. Hepatitis A (formerly called infectious hepatitis) was first differentiated epidemiologically from hepatitis B, which has a long incubation period, in the 1940s. Development of serologic tests allowed definitive diagnosis of hepatitis B. In the 1970s, identification of the virus, and development of serologic tests helped differentiate hepatitis A from other types of non-B hepatitis.[5]
Until 2004, HAV was the most frequently reported type of hepatitis in the United States. In the pre-vaccine era, the primary methods used for preventing HAV infections were hygienic measures and passive protection with immune globulin (IG). HAV vaccines were licensed in 1995 and 1999. These vaccines provide long-term protection against HAV infection.[6]
HAV is the only common vaccine-preventable foodborne disease in the United States.[7] This virus is one of five human hepatitis viruses that primarily infect the human liver and cause human illness.[8] Unlike hepatitis B and C, HAV does not develop into chronic hepatitis or cirrhosis, which are both potentially fatal conditions.[9] Nonetheless, infection with the HAV virus can lead to acute liver failure and death.[10]
Where does Hepatitis A Come From?
HAV is a communicable (or contagious) disease that often spreads from person to person.[11] Person-to-person transmission occurs via the “fecal-oral route,” while all other exposure is generally attributable to contaminated food or water.[12] Food-related outbreaks are usually associated with contamination of food during preparation by a HAV-infected food handler.[13] The food handler is generally not ill because the peak time of infectivity—that is, when the most virus is present in the stool of an infected individual—occurs two weeks before illness begins.[14]
Fresh produce contaminated during cultivation, harvesting, processing, and distribution has also been a source of HAV.[15] In 1997, frozen strawberries were the source of a HAV outbreak in five states.[16] Six years later, in 2003, fresh green onions were identified as the source of a HAV outbreak traced to consumption of food at a Pennsylvania restaurant.[17] Other fruits and vegetables, such as blueberries and lettuce, have also been associated with HAV outbreaks in the U.S., as well as in other developed countries.[18] HAV is relatively stable and can survive for several hours on fingertips and hands, and up to two months on dry surfaces.[19] The virus can be inactivated by heating to 185°F (85°C) or higher for one minute, or disinfecting surfaces with a 1:100 dilution of household bleach in tap water.[20] HAV can still be spread from cooked food if it is contaminated after cooking.[21]
Although ingestion of contaminated food is a common means of spread for HAV, it may also be spread by household contact among families or roommates, sexual contact, or by direct inoculation from persons sharing illicit drugs.[22] Children are often asymptomatic, or have unrecognized infections, and can pass the virus through ordinary play, unknown to their parents, who may later become infected from contact with their children.[23]
What are the Symptoms of Hepatitis A?
HAV may cause no symptoms at all when it is contracted, especially in children.[24] Asymptomatic individuals will only know they were infected (and have become immune, given that you can only get HAV once) by getting a blood test later in life.[25] Approximately 10 to 12 days after exposure, HAV is present in blood and is excreted via the biliary system into the feces.[26] Although the virus is present in the blood, its concentration is much higher in feces.[27] HAV excretion begins to decline at the onset of clinical illness, and decreases significantly by seven to ten days after onset of symptoms.[28] Most infected persons no longer excrete virus in the feces by the third week of illness. Children may excrete HAV longer than adults.[29]
Seventy percent of HAV infections in children younger than six years of age are asymptomatic; in older children and adults, infection tends to be symptomatic with more than 70% of those infected developing jaundice.[30] Symptoms typically begin about 28 days after contracting HAV, but can begin as early as 15 days or as late as 50 days after exposure.[31] The symptoms include muscle aches, headache, anorexia (loss of appetite), abdominal discomfort, fever, and malaise.[32]
After a few days of typical symptoms, jaundice (also termed “icterus”) sets in.[33] Jaundice is a yellowing of the skin, eyes, and mucous membranes that occurs because bile flows poorly through the liver and backs up into the blood.[34] The urine will also turn dark with bile and the stool light or clay-colored from lack of bile.[35] When jaundice sets in, initial symptoms such as fever and headache begin to subside.[36]
In general, symptoms usually last less than two months, although 10% to 15% of symptomatic persons have prolonged or relapsing disease for up to six months.[37] It is not unusual, however, for blood tests to remain abnormal for six months or more.[38] The jaundice so commonly associated with HAV can also linger for a prolonged period in some infected persons, sometimes as long as eight months or more.[39] Additionally, pruritus—or severe “itchiness” of the skin—can persist for several months after the onset of symptoms. These conditions are frequently accompanied by diarrhea, anorexia, and fatigue.[40]
Relapse is possible with HAV, typically within three months of the initial onset of symptoms.[41] Although relapse is more common in children, it does occur with some regularity in adults.[42] The vast majority of persons who are infected with HAV fully recover, and do not develop chronic hepatitis.[43] Persons do not carry HAV long-term, as with hepatitis B and C.[44]
Fulminant Hepatitis A
Fulminant hepatitis A, or acute liver failure, is a rare but devastating complication of HAV infection.[45] As many as 50% of individuals with acute liver failure may die or require emergency liver transplantation.[46] Elderly patients and patients with chronic liver disease are at higher risk for fulminant hepatitis A.[47] In parallel with a declining incidence of acute HAV infection in the general population, the incidence of fulminant hepatitis A appears to be decreasing.[48]
HAV infects the liver’s parenchymal cells (internal liver cells).[49] Once a cell has been penetrated by the viral particles, the HAV releases its own toxins that cause, in essence, a hostile takeover of the host’s cellular system.[50] The cell then produces new viral components that are released into the bile capillaries or tubes, which run between the liver’s parenchymal cells.[51] This process results in the death of liver cells, called hepatic necrosis.[52]
The fulminant form of hepatitis occurs when this necrotic process kills so many liver cells—upwards of three-quarters of the liver’s total cell count—that the liver can no longer perform its job.[53] Aside from the loss of liver function, fulminant hepatic failure can lead to encephalopathy and cerebral edema.[54] Encephalopathy is a brain disorder that causes central nervous system depression and abnormal neuromuscular function.[55] Cerebral edema is a swelling of the brain that can result in dangerous intracranial pressure.[56] Intracranial hypertensions, leading to a brain stem death and sepsis with multiple organ failure, are the leading causes of death in individuals with fulminant hepatic failure.[57]
Incidence of Hepatitis A Infection
HAV is much more common in countries with underdeveloped sanitation systems and, thus, is a risk in most of the world.[58] An increased transmission rate is seen in all countries other than the United States, Canada, Japan, Australia, New Zealand, and Western European countries.[59] Nevertheless, infections continue to occur in the United States, where approximately one-third of the population has been previously infected with HAV.[60]
Each year, approximately 30,000 to 50,000 cases of HAV occur in the United States.[61] Historically, acute HAV rates have varied cyclically, with nationwide increases every 10 to 15 years.[62] The national rate of HAV infections has declined steadily since the last peak in 1995.[63] Although the national incidence—1.0 case per 100,000 population—of HAV was the lowest ever recorded in 2007, it is estimated that asymptomatic infections and underreporting kept the documented incidence-rate lower than it actually is. In fact, 25,000 new infections were estimated in 2007.[64]
In 2007, the CDC reported a total of 2,979 acute symptomatic cases of HAV.[65] Of these, information about food and water exposure was known for 1,047 cases, leading to an estimate that 6.5% of all infections were caused by exposure to contaminated water or food.[66] In 2,500 of the cases, no known risk factor was identified.[67]
Hepatitis A outbreaks associated with fresh, frozen, and minimally processed produce, worldwide, from 1983 to 2016
| Year | # Cases | Implicated food | Location of cases | Source of implicated food | Suspected cause of contamination | Reference |
| 1983 | 24 | Raspberries (frozen) | Scotland | Scotland | Infected pickers or packers | Reid et al., 1987[68] |
| 1987 | 5 | Raspberries (frozen) | Scotland | Tayside, Scotland | Infected pickers | Ramsay and Upton, 1989[69] |
| 1988 | 202 | Iceberg lettuce | Kentucky | Unknown, suspected to be from Mexico | Believed to have occurred prior to distribution, since multiple restaurants involved | Rosenblum et al., 1990[70] |
| 1990 | 35 | Strawberries (frozen) | Montana, Georgia | California | Suspect an infected picker at farm | Sivapalasingam et al., 2004;[71]Niu et al., 1992[72] |
| 1996 | 30 | Salad ingredients | Finland | Imported salad ingredients | Unknown | Pebody et al., 1998[73] |
| 1997 | 256 | Strawberries (frozen) | Michigan, Maine, Wisconsin, Arizona, Louisiana, Tennessee | Grown in Mexico,processed and frozen at a single California facility a year before consumption | Inconclusive due to time between harvest and consumption, suspect barehanded contact with berries at harvesting, coupled with few latrines and handwashing facilities on site | Hutin et al., 1999[74] |
| 1998 | 43 | Green onions | Ohio | One of two Mexican farms or a farm in California | Believed to be contaminated before arrival at restaurant | Dentinger et al., 2001[75] |
| 2000 | 31 | Green onions or tomatoes | Kentucky, Florida | Green onions: California or MexicoTomatoes: Unknown | Unknown | Wheeler et al., 2005[76]; Datta et al., 2001[77]; Fiore, 2004[78] |
| 2002 | 81 | Blueberries | New Zealand | New Zealand, one orchard | Inadequate bathroom facilities in fields, workers had barehanded contact with product, polluted groundwater from nearby latrines a possibility | Calder et al., 2003[79] |
| 2003 | 601 | Green onions | Pennsylvania, Tennessee, Georgia, North Carolina | Mexico, two farms | Contaminated during or before packing at farm | CDC, 2003[80]; Wheeler et al., 2005[81] |
| 2009 | 562 | Tomatoes | Australia | Unknown; imported and domestic product involved | Product suspected to be imported due to concurrent outbreaks elsewhere at the time, source of contamination unknown | Donnan et al., 2012[82] |
| 2009 | 13 | Tomatoes | Netherlands | Unknown; imported product suspected | Identical strain to the 2009 Australian outbreak | Petrignani et al., 2010[83] |
| 2010 | 59 | Tomatoes | France | Likely Turkey, single batch of product | Unable to determine when and where contamination occurred. Virus was slightly different from one in the 2009 Australian and Dutch outbreaks. | Gallot et al., 2011[84] |
| 2012 | 9 | Pomegranate seeds (frozen) | Canada | Egypt | Suspect product contamination before export. Some history of travel to endemic areas among workers at Canadian processing facility, but less likely as only one product was associated with illness. | CDC 2013[85]; Swinkels et al., 2014[86] |
| 2013 | 103 | Strawberries (frozen)Other frozen berries may have been involved | Denmark, Finland, Norway, Sweden | Suspected Egypt and Morocco based on virus strain and import history | Unknown, some cases matched the strain of the larger 2013 European outbreak (see below) | Nordic Outbreak Investigation Team, 2013[87] |
| 2013 | 1589 | Berries (frozen) | Italy (90% of cases), Austria, Bulgaria, Denmark, England, Finland, France, Germany, Ireland, the Netherlands, Norway, Poland, Sweden | Multiple food items containing frozen mixed berries (cakes, smoothies); Bulgarian blackberries and Polish redcurrants were the most common ingredients in the implicated lots | Unknown, no single source found. Some cases also related to travel to Italy. | Severi et al., 2015[88]; EFSA 2014[89]; Chiapponi et al., 2014[90]; Rizzo et al., 2013[91]; Guzman-Herrador et al., 2014[92]; Fitzgerald et al., 2014[93] |
| 2013 | 165 | Pomegranate arils (frozen) | Arizona, California, Colorado, Hawaii, New Hampshire, New Jersey, New Mexico, Nevada, Utah, Wisconsin | Turkey | Unknown | Collier et al., 2014[94]; CDC 2013[95] |
| 2016 | 143 | Strawberries (frozen) | Arkansas, California, Maryland, New York, North Carolina, Oregon, Virginia, West Virginia, Wisconsin | Egypt | Unknown | CDC 2016[96] |
Estimates of the annual costs (direct and indirect) of HAV in the United States have ranged from $300 million to $488.8 million in 1997 dollars.[97] In one study conducted in Spokane, Washington, the combined direct and indirect costs for each case of HAV, from all sources, ranged from $2,892 to $3,837.[98] In a 2007 Ohio study, each case of HAV infection attributable to contaminated food was estimated to cost at least $10,000, including medical and other non-economic costs.[99] Nationwide, adults who become ill miss an average of 27 workdays per illness, and 11% to 22% of those infected are hospitalized.[100] All of these costs are entirely preventable, given the effectiveness of a vaccination in providing immunity from infection.[101]
[1] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” in Mandell, Douglas, & Bennett’s PRINCIPLES AND PRACTICE OF INFECTIOUS DISEASES, Fifth Edition, Chap. 161, pp. 1920-40 (2000); Mayo Clinic Staff, “Hepatitis A,” (last updated Sept 1, 2011). Articles available online at http://www.mayoclinic.com/health/hepatitis-a/DS00397.
[2] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[3] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[4] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[5] CDC, “Hepatitis A,” in EPIDEMIOLOGY AND PREVENTION OF VACCINE-PREVENTABLE DISEASES (also known as “The Pink Book”), Atkinson W, Wolfe S, Hambrosky J, McIntyre L, editors, 12th edition. Chapter available online at http://www.cdc.gov/vaccines/pubs/pinkbook/hepa.html.
[6] Id.
[7] Id.; See also Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” Clinical Infectious Diseases, Vol. 38, 705-715 (March 1, 2004). Full text online at http://www.cdc.gov/hepatitis/PDFs/fiore_ha_transmitted_by_food.pdf.
[8] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[9] Id.
[10] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[11] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[12] Id.; See also Jaykus Lee Ann, “Epidemiology and Detection as Options for Control of Viral and Parasitic Foodborne Disease,” Emerging Infectious Diseases, Vol. 3, No. 4, pp. 529-39 (October-December 1997). Full text of the article is available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2640072/pdf/9366607.pdf
[13] Fiore, Anthony, supra note 7; CDC, “Hepatitis A,” supra note 5; See also CDC, “Surveillance for Acute Viral Hepatitis – United States, 2007, Morbidity and Mortality Weekly Report, Surveillance Summaries, Vol. 58, No. SS03 (May 22, 2009) at http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5803a1.htm.
[14] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7.
[15] Id.; See also, Wheeler, C, et al., “An Outbreak of Hepatitis A Associated with Green Onions,” New England Journal of Medicine, Vol. 353, 890-97 (2005). Full text of article available at http://www.nejm.org/doi/full/10.1056/NEJMoa050855.
[16] Hutin YJF, et al., “A Multistate, Foodborne Outbreak of Hepatitis A,” New England Journal of Medicine, Vol. 340, pp. 595-602 (1999). Full text of article is online at http://nejm.org/doi/full/10.1056/NEJM199902253400802.
[17] Wheeler, C, et al., “An Outbreak of Hepatitis A Associated with Green Onions,” supra note 15.
[18] Butot S, et al., “Effects of Sanitation, Freezing and Frozen Storage on Enteric Viruses in Berries and Herbs,” Intentional Journal of Food Microbiology, Vol. 126, No. 4, pp. 233-246 (2003). Full text of article is available at http://www.prograd.uff.br/virologia/sites/default/files/bulot_et_al_2008_inactivation.pdf.; Calder, L, et al., An Outbreak of Hepatitis A Associated with Consumption of Raw Blueberries,” Epidemiology and Infection, Vol. 131, No. 1 745-51 (2003) at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2870016/pdf/12948375.pdf.
[19] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[20] CDC, “Updated recommendations from Advisory Committee on Immunization Practices (ACIP) for use of hepatitis A vaccine in close contacts of newly arriving international adoptees,” Morbidity and Mortality Weekly Report, Vol. 58, No. 36, (Sept. 18, 2006), http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5836a4.htm; Fiore, Anthony, et al., Advisory Committee on Immunization Practices (ACIP), Prevention of Hepatitis-A Through Active or Passive Immunization: Recommendations, Morbidity & Mortality Weekly Review, Vol. 55, Report 407, (May 29, 2006) at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5507a1.htm; Todd, Ewan C.D., et al., “Outbreaks Where Food Workers Have Been Implicated in the Spread of Foodborne Disease. Part 6. Transmission and Survival of Pathogens in the Food Processing and Preparation-environment,” Journal of Food Protection, Vol. 72, 202-19 (2009). Full text of the article is available online at http://courses.washington.edu/eh451/articles/Todd_2009_food%20processing.pdf.
[21] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7.
[22] Id.; See also, Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[23] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Piazza, M, et al., “Safety and Immunogenicity of Hepatitis A Vaccine in Infants: A Candidate for Inclusion in Childhood Vaccination Program,” Vol. 17, pp. 585-588 (1999). Abstract at http://www.ncbi.nlm.nih.gov/pubmed/10075165; Schiff, E.R., “Atypical Manifestations of hepatitis-A,” Vaccine, Vol. 10, Suppl. 1, pp. 18-20 (1992). Abstract at http://www.ncbi.nlm.nih.gov/pubmed/1475999.
[24] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7
[25] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[26] CDC, “Hepatitis A,” supra note 5; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1
[27] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1
[28] Id.
[29] Id.; See also Sagliocca, Luciano, et al., “Efficacy of Hepatitis A Vaccine in Prevention of Secondary Hepatitis A Infection: A Randomized Trial,” Lancet, Vol. 353, 1136-39 (1999). Abstract at http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(98)08139-2/abstract.
[30] CDC, “Hepatitis A,” supra note 5.
[31] Id.; See also Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7.
[32] CDC, “Hepatitis A,” supra note 5; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[33] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[34] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[35] CDC, “Hepatitis A,” supra note 5; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[36] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[37] Fiore, Anthony, et al., Advisory Committee on Immunization Practices (ACIP), Prevention of Hepatitis-A Through Active or Passive Immunization: Recommendations,” supra note 20; Gilkson Miryam, et al., “Relapsing Hepatitis A. Review of 14 cases and literature survey,” Medicine, Vol. 71, No. 1, 14-23 (Jan. 1992). Abstract of article online at http://www.ncbi.nlm.nih.gov/pubmed/1312659.
[38] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[39] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[40] CDC, “Hepatitis A,” supra note 5; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[41] Gilkson Miryam, et al., “Relapsing Hepatitis A. Review of 14 cases and literature survey,” supra note 37.
[42] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Gilkson Miryam, et al., “Relapsing Hepatitis A. Review of 14 cases and literature survey,” supra note 37.
[43] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[44] CDC Summary, “Disease Burden from Viral Hepatitis A, B and C in the United States, 2004-2009, at http://www.cdc.gov/hepatitis/pdfs/disease_burden.pdf; CDC, “Hepatitis A,” supra note 5.
[45] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” World Journal of Gastroenterology, Vol. 12, No. 46 pp. 7405-7412 (Dec. 14, 2006). Full article is available online at http://www.wjgnet.com/1007-9327/12/7405.pdf.
[46] Taylor, Ryan, et al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” Hepatology, Vol. 44, 1589-1597. Full text http://deepblue.lib.umich.edu/bitstream/2027.42/55879/1/21349_ftp.pdf.
[47] Id.; See also Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[48] Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.
[49] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[50] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Schiff, E.R., “Atypical Manifestations of hepatitis-A,” supra note 23.
[51] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45.
[52] Id.; See also Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.
[53] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45; Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.
[54] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45.
[55] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[56] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45.
[57] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45; Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.
[58] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Jaykus Lee Ann, “Epidemiology and Detection as Options for Control of Viral and Parasitic Foodborne Disease,” supra note 12.
[59] CDC, “Update: Prevention of Hepatitis A after Exposure to Hepatitis A Virus and in International Travelers, Updated ACIP Recommendations,” Morbidity and Mortality Weekly Report, Vol. 56, No. 41, pp. 1080-84 (Oct. 19, 2007), online at http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5641a3.htm.
[60] CDC, “Surveillance for Acute Viral Hepatitis – United States 2007,” supra note 13; Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7.
[61] CDC, Summary, “Disease Burden from Viral Hepatitis A, B, and C in the United States,” supra note 44; CDC, “Hepatitis A,” supra note 5.
[62] Hutin YJF, et al., “A Multistate, Foodborne Outbreak of Hepatitis A,” supra note 16.
[63] CDC, Summary, “Disease Burden from Viral Hepatitis A, B, and C in the United States,” supra note 44; CDC, “Surveillance for Acute Viral Hepatitis – United States 2007,” supra note 13.
[64] CDC, “Surveillance for Acute Viral Hepatitis – United States 2007,” supra note 13; Schiff, E.R., “Atypical Manifestations of hepatitis-A,” supra note 23.
[65] CDC, “Surveillance for Acute Viral Hepatitis – United States 2007,” supra note 13.
[66] Id.
[67] Id.
[68] Reid, T., Robinson, H. (1987). Frozen raspberries and hepatitis A. Epidemiol Infect, 98: 109–112.
[69] Ramsay, C. N. and Upton, P. A. (1989). Hepatitis A and frozen raspberries. Lancet, 1: 43–44.
[70] Rosenblum, L. S., Mirkin, I. R., Allen, D. T., Safford, S., Hadler, S. C. (1990). A multifocal outbreak of hepatitis A traced to commercially distributed lettuce. American Journal of Public Health, 80(9): 1075-1079.
[71] Sivapalasingam, S., Friedman, C. R., Cohen, L., Taube, R. V. (2004). Fresh produce: a growing cause of outbreaks of foodborne illness in the United States, 1973 through 1997. J Food Prot, 67: 2342-2353.
[72] Niu, M. T., Polish, L. B., Robertson, B. H. (1992). Multistate outbreak of hepatitis A associated with frozen strawberries. J Infect Dis 166: 518-524.
[73] Pebody, R. G., Leino, T., Ruutu, P., Kinnunen, L., Davidkin, I., Nohynek, H., & Leinikki, P. (1998). Foodborne outbreaks of hepatitis A in a low endemic country: an emerging problem? Epidemiology and infection, 120(1): 55-59.
[74] Hutin, Y. J., Pool, V., Cramer, E. H., Nainan, O. V., Weth, J., Williams, I. T. et al. (1999). A multistate, foodborne outbreak of hepatitis A. New England Journal of Medicine, 340(8): 595-602.
[75] Dentinger, C. M., Bower, W. A., Nainan, O. V., Cotter, S. M., Myers, G., Dubusky, L. M., Fowler, S., Salehi, E. D. P., and Bell, B. P. (2001). An outbreak of hepatitis A associated with green onions. J Infect Dis, 183: 1273-1276.
[76] Wheeler, C., Vogt, T. M., Armstrong, G. L., Vaughan, G., Weltman, A., Nainan, O. V. et al. (2005). An outbreak of hepatitis A associated with green onions. New England Journal of Medicine, 353(9): 890-897.
[77] Datta, S. D., Traeger, M. S., & Nainan, O. V. (2001). Identification of a multi-state outbreak of hepatitis A associated with green onions using a novel molecular epidemiologic technique [abstract 896]. In Program and abstracts of the 39th Annual Meeting of the Infectious Diseases Society of America. Alexandra, VA: Infectious Diseases Society of America (Vol. 192).
[78] Fiore, A. E. (2004). Hepatitis A transmitted by food. Clinical Infectious Diseases, 38(5): 705-715.
[79] Calder, L. , Simmons, G., Thornley, G. (2003). An outbreak of hepatitis A associated with consumption of raw blueberries. Epidemiol Infect,131: 745-751
[80] Centers for Disease Control and Prevention (CDC). (2003). Hepatitis A outbreak associated with green onions at a restaurant–Monaca, Pennsylvania, 2003. MMWR, 52(47): 1155-1157. Available at https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5247a5.htm
[81] Wheeler, C., Vogt, T. M., Armstrong, G. L., Vaughan, G., Weltman, A., Nainan, O. V. et al. (2005). An outbreak of hepatitis A associated with green onions. New England Journal of Medicine, 353(9): 890-897.
[82] Donnan, E. J., Fielding, J. E., Gregory, J. E., et al. (2012). A multistate outbreak of hepatitis A associated with semidried tomatoes in Australia, 2009. Clin Infect Dis, 54: 775–781.
[83] Petrignani, M., Harms, M., Verhoef, L. (2010). Update: a food-borne outbreak of hepatitis A in The Netherlands related to semi-dried tomatoes in oil, January-February 2010. Euro Surveillance, 15(20): 19572.
[84] Gallot, C., Grout, L., Roque-Afonso, A., Couturier, E., Carrillo-Santisteve, P., Pouey, J. et al. (2011). Hepatitis A Associated with Semidried Tomatoes, France, 2010. Emerging Infectious Diseases, 17(3): 566-567.
[85] Centers for Disease Control and Prevention (CDC). (2013). Multistate outbreak of hepatitis A virus infections linked to pomegranate seeds from Turkey (Final Update). Available at: https://www.cdc.gov/hepatitis/outbreaks/2013/a1b-03-31/
[86] Swinkels, H. M., Kuo, M., Embree, G., Andonov, A., Henry, B., Buxton, J. A. (2014). Hepatitis A outbreak in British Columbia, Canada: the roles of established surveillance, consumer loyalty cards and collaboration, February to May 2012. Euro Surveillance, 19: 20792.
[87] Nordic Outbreak Investigation Team C (2013). Joint analysis by the Nordic countries of a hepatitis A outbreak, October 2012 to June 2013: frozen strawberries suspected. Euro Surveillance, 18(27): 20520.
[88] Severi, E., Verhoef, L., Thornton, L., Guzman-Herrador, B. R., Faber, M., Sundqvist, L. et al. (2015). Large and prolonged food-borne multistate hepatitis A outbreak in Europe associated with consumption of frozen berries, 2013 to 2014. Euro Surveillance, 20(29): 1-9.
[89] European Food Safety Authority (EFSA). (2014). Tracing of food items in connection to a multinational hepatitis A virus outbreak in Europe. EFSA Journal, 12(9): 3821-4007. Available at http:// www.efsa.europa.eu/en/efsajournal/pub/3821.htm
[90] Chiapponi, C., Pavoni, E., Bertasi, B., Baioni, L., Scaltriti, E., Chiesa, E., et al. (2014). Isolation and genomic sequence of hepatitis A virus from mixed frozen berries in Italy. Food Environ Virol, 6(3): 202-206.
[91] Rizzo, C., Alfonsi, V., Bruni, R., Busani, L., Ciccaglione, A., De Medici, D., et al. (2013). Ongoing outbreak of hepatitis A in Italy: preliminary report as of 31 May 2013. Euro Surveillance, 18(27): 20518.
[92] Guzman-Herrador, B., Jensvoll, L., Einoder-Moreno, M., Lange, H., Myking, S., Nygard, K., et al. (2014). Ongoing hepatitis A outbreak in Europe 2013 to 2014: imported berry mix cake suspected to be the source of infection in Norway. Euro Surveillance, 19(15): 20775.
[93] Fitzgerald, M., Thornton, L., O’Gorman, J., O Connor, L., Garvey, P., Boland, M., et al. (2014). Outbreak of hepatitis A infection associated with the consumption of frozen berries, Ireland, 2013 – linked to an international outbreak. Euro Surveillance: European communicable disease bulletin, 19(43).
[94] Collier, M. G., Khudyakov, Y. E., Selvage, D., Adams-Cameron, M., Chiepson, E., Cronquist, A., et al. (2014). Outbreak of hepatitis A in the USA associated with frozen pomegranate arils imported from Turkey: an epidemiological case study. Lancet Infectious Diseases, 14(10): 976-981.
[95] Centers for Disease Control and Prevention (CDC). (2013) – Multistate outbreak of hepatitis A virus infections linked to pomegranate seeds from Turkey (Final Update), supra note 85.
[96] Centers for Disease Control and Prevention (CDC). (2016). 2016 – Multistate outbreak of hepatitis A linked to frozen strawberries (Final Update). Available at https://www.cdc.gov/hepatitis/outbreaks/2016/hav-strawberries.htm
[97] CDC, Summary, “Disease Burden from Viral Hepatitis A, B, and C in the United States,” supra note 44.
[98] Bownds, Lynne, et al., “Economic Impact of a Hepatitis A Epidemic in a Mid-Sized Urban Community: The Case of Spokane, Washington,” Journal of Community Health, Vol. 28, No. 4, pp. 233-46 (2003). Abstract at http://www.ncbi.nlm.nih.gov/pubmed/12856793; Fiore, Anthony, et al., Advisory Committee on Immunization Practices (ACIP), Prevention of Hepatitis-A Through Active or Passive Immunization: Recommendations,” supra note 20.
[99] Scharff, RL, et al., “Economic Cost of Foodborne Illness in Ohio,” Journal of Food Protection, Vol. 72, No. 1, pp. 128-36 (2009). Abstract available online at http://www.ingentaconnect.com/content/iafp/jfp/2009/00000072/00000001/art00018.
[100] CDC, “Surveillance for Acute Viral Hepatitis – United States 2007,” supra note 13; CDC, “Hepatitis A,” supra note 5.
[101] CDC, “Hepatitis A,” supra note 5; Fiore, Anthony, et al., Advisory Committee on Immunization Practices (ACIP), Prevention of Hepatitis-A Through Active or Passive Immunization: Recommendations,” supra note 20.

No details about those sickened, no details about the grower, processor or seller, and no details about the conditions that allowed for the contamination? Where is the “root cause analysis?”
I have a word for the FDA and CDC – “Transparency.”
Thanks to Food Safety News for reporting this out:
The FDA has determined an outbreak of infections from Salmonella Typhimurium was from contaminated cantaloupe and declared its investigation over.
First posted on Aug. 17 by the Food and Drug Administration, there has been little information available on the outbreak, except for the patient count, which currently stands at 87. The agency did not report the ages of the patients or their states of residence.
At the first posting, there were 44 confirmed patients. The source of the Salmonella was listed as unknown from Aug. 17 to Oct. 5.
The FDA has been working on traceback, testing and on-site inspections for weeks, but did not reveal what food was being traced. On Oct. 5 it announced that the investigation had determined cantaloupe was the source of the pathogen.
The agency did not report whether the cantaloupe involved was whole fruit or fresh-cut. It also did not reveal a grower, packer, distributor or retailers where the cantaloupe was produced and sold.
“The vehicle of the outbreak was confirmed after the outbreak ended. Given the product(s) were no longer on the market, there was no ongoing risk to public health and no need to avoid eating cantaloupe. Additional information on this outbreak will be forthcoming,” according to the FDA.
The FDA did not report when the implicated cantaloupe was no longer available to the public.

The Michigan Department of Agriculture and Rural Development (MDARD) is advising consumers not to eat any Kuntry Gardens produce or products containing produce from Kuntry Gardens of Homer, MI, as it may be contaminated with raw, untreated human waste. All product is expected to be labeled under the name Kuntry Gardens.
During a routine produce safety inspection, MDARD staff identified that Kuntry Gardens was using raw, untreated human waste on the fields where produce was grown for sale to local grocery stores and direct sale. Use of raw, untreated, human waste for growing commodities intended for human food is a violation of the Michigan Food Law, PA 92 of 2000, as well as other state and federal laws and regulations.
No illnesses have been reported to date; however, MDARD is urging any individuals experiencing symptoms such as nausea, vomiting, diarrhea, jaundice (yellowing of the skin), fever, abdominal cramps, loss of appetite, weakness, headache, or other symptoms of foodborne illness to seek medical advice.
If not treated professionally, human waste and other body fluids can spread dangerous infectious diseases such as hepatitis A, Clostridium difficile, E coli, rotavirus and norovirus.
Product may have been further distributed or sold at additional locations, but is known to have been sold at the following locations in Michigan:
• Kuntry Gardens, 29910 R Dr South, Homer
• Busch’s Fresh Food Market stores located in Ann Arbor, Brighton, Canton, Clinton, Dexter, Farmington Hills, Livonia, Novi, Pinckney, Plymouth-Northville, Rochester Hills, Saline, South Lyon, Tecumseh, and West Bloomfield
• Simply Fresh Market, 7300 Grand River Rd, Brighton
• White Lotus, 7217 W Liberty Rd, Ann Arbor
• Argus Farm Stop, 325 W Liberty Street, Ann Arbor
• Agricole Farm Stop, 118 N Main Street, Chelsea
• Pure Pastures, 1192 Ann Arbor Rd, Plymouth
• Ypsi Coop, 312 North River Street, Ypsilanti
• Greener Pastures Market, 21202 Pontiac Trail, South Lyon
• Holiday Market, 520 S Lilley Rd, Canton
• Cherry Capitol, Traverse City
MDARD has placed impacted product still on the farm under seizure and is working with the farm to oversee disposition and corrective action.
