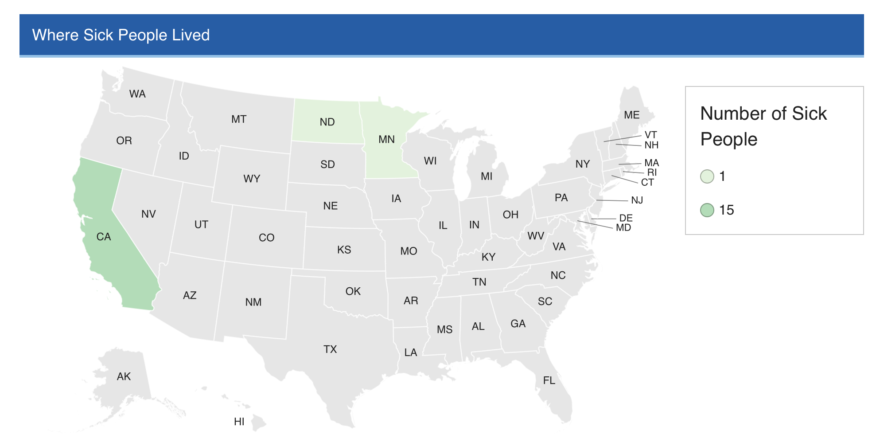
CDC, public health and regulatory officials in several states, and the U.S. Food and Drug Administration are investigating a multistate outbreak of hepatitis A potentially linked to contaminated fresh organic strawberries reportedly sold as FreshKampo or HEB, purchased in the United States between March 5, 2022, and April 25, 2022. The Public Health Agency of Canada and the Canadian Food Inspection Agency are also investigating an outbreak of hepatitis A; imported fresh organic strawberries have been identified as the likely source of that outbreak. Traceback investigations show that outbreak-associated cases in California, Minnesota, and Canada report having purchased fresh organic strawberries prior to becoming ill.
As of May 31, 2022, in the United Sates, a total of 17 outbreak-associated cases of hepatitis A have been reported from 3 states.
Illnesses started on dates ranging from March 28, 2022, to April 30, 2022. Ill people range in age from 9 to 73 years, with a median age of 58. Seventy-one percent of ill people are female. Of 17 people with available information, 12 (71%) have been hospitalized. No deaths have been reported.

Epidemiologic and traceback evidence indicate that fresh organic strawberries are a likely source of this outbreak. The potentially affected FreshKampo and HEB products are past shelf life and no longer available for purchase in the United States. People who purchased FreshKampo or HEB fresh organic strawberries between March 5, 2022, and April 25, 2022 and then froze those strawberries for later consumption should not eat them. These products may have been sold at the following retailers, including, but not limited to: HEB, Kroger, Safeway, Sprouts Farmers Market, Trader Joe’s, Walmart, Weis Markets, and WinCo Foods.
In Canada, as of June 2, 2022, there are 10 laboratory-confirmed cases of hepatitis A illness being investigated in two provinces: Alberta (4) and Saskatchewan (6). Individuals became ill between early and mid April 2022. Individuals who became ill are between 10 to 75 years of age. Four individuals have been hospitalized. No deaths have been reported.
The CFIA is conducting a food safety investigation into the FreshKampo brand fresh organic strawberries purchased between March 5 and 9, 2022 at Co-op stores in Alberta and Saskatchewan. Currently, there are no food recall warnings associated with this outbreak.
In interviews, ill people answered questions about the foods they ate and other exposures in the 2 to 7 weeks before they became ill. Of people who were interviewed, 10/13 (77%) reported eating fresh organic strawberries. This proportion was significantly higher than results from a survey of healthy people in which 50% reported eating fresh strawberries in the week before they were interviewed.
Currently, the potentially affected FreshKampo and HEB products are past shelf life. People who purchased FreshKampo and HEB fresh organic strawberries between March 5, 2022, and April 25, 2022, and then froze those strawberries for later consumption should not eat them. These products were sold at the following retailers, including, but not limited to:
Aldi
HEB
Kroger
Safeway
Sprouts Farmers Market
Trader Joe’s
Walmart
Weis Markets
WinCo Foods
Canadian Co-op stores

Contact your healthcare provider if you think you may have symptoms of a hepatitis A infection after eating these fresh organic strawberries, or if you believe that you have eaten these strawberries in the last two weeks. If you have eaten these organic strawberries, purchased fresh and later frozen, or have symptoms consistent with hepatitis A, see your health care provider immediately. Vaccination can prevent a hepatitis A infection if given within 14 days of exposure. Symptoms of hepatitis A include:
fever
dark urine
loss of appetite
fatigue (tiredness)
nausea and vomiting
stomach cramps or abdominal pain
jaundice (yellowing of the skin and eyes)
After you have been exposed to hepatitis A, symptoms typically appear 14 to 28 days later, but may occur up to 50 days later.
Symptoms usually last less than two months. Mild symptoms may last only one or two weeks, while severe symptoms can last up to nine months.
Anyone can become ill with hepatitis A infection. Most people who become ill from a hepatitis A infection will recover fully, but the risk of serious complications increases with older age and in those with underlying liver disease.
It is possible for some people to be infected with hepatitis A and to not get ill or show any symptoms, but to still be able to spread the virus to others.
Wash and sanitize any drawers, shelves, or containers where the products were stored using a kitchen sanitizer (follow the directions on the container) or prepare a bleach solution in a labelled spray bottle (you can use a ratio of 5 ml of household bleach to 750 ml of water) and rinse with water.
Wash your hands before and after preparing or eating food, and after using the washroom or changing diapers.
If you have been diagnosed with hepatitis A, do not prepare or serve food and drinks to others.