Infant botulism from powdered formula was not a freak accident. It was foreseeable — and the people who could have prevented it chose to wait for sick babies instead.
For over thirty years I have heard the same line from every defendant: nobody could have seen this coming.
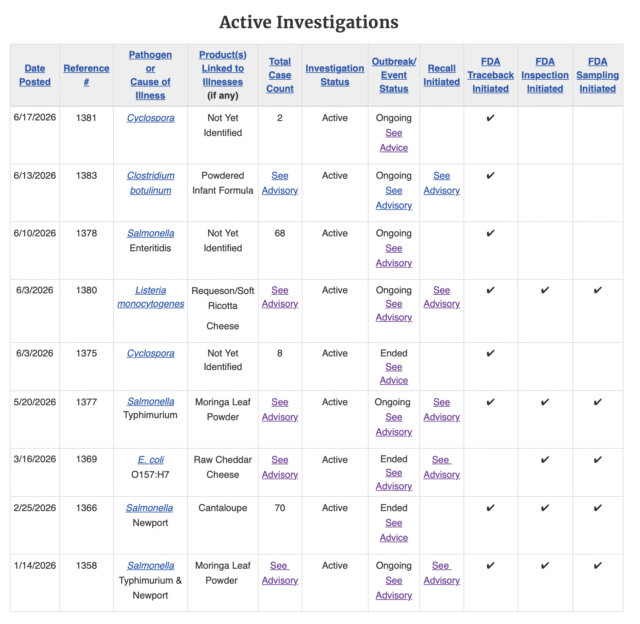
Over the past year, two powdered infant formulas gave babies botulism. By CDC’s accounting, ByHeart’s Whole Nutrition formula sickened 48 infants across 17 states. Months later, Nara Organics’ Whole Milk Organic formula sickened three more in California, Pennsylvania, and Washington. These are not statistics. They are babies who went limp, stopped sucking, stopped breathing, and spent weeks in hospitals on a drug called BabyBIG — an antitoxin made from human plasma — because spores of Clostridium botulinum germinated in guts too young to fight them off.
The hazard was known. The pathway was known. The fix was available. And the government’s own record proves it.
Start with the international authorities. In 2004, a joint FAO/WHO expert meeting sorted the microbes that can ride along in powdered infant formula by how strong the evidence was that each one made babies sick. They put Clostridium botulinum in the bottom category: “causality less plausible or not yet demonstrated.” Read that again. The world’s food-safety experts found botulism in the product and filed it under not yet.
Not yet is not, not, a risk.
The same report admitted the uncomfortable truth at the center of this whole business: powdered infant formula “is not a sterile product and may occasionally contain pathogens.” Codex followed in 2008 and declined to treat botulism as a hazard in infant formula at all. The international microbiology body followed in 2014 and recommended that manufacturers not even bother routinely testing for it.
Meanwhile, the science on where these spores come from was sitting in plain sight. A 2010 peer-reviewed review laid out the entire chain: C. botulinum lives in soil and silage, cattle pick it up, the spores pass into raw milk, and — this is the part that matters — ordinary pasteurization does not kill them. Dry that milk into powder, and the spores are concentrated and come along for the ride into the can.
The dairy industry knew it, too. For years it ran funded “low-spore milk powder” programs, set numerical spore tolerances, and taught processors to keep spores out starting at the farm gate. They built the entire playbook — for taste and shelf life. They simply never ran it for the one spore that paralyzes infants.
And then there is the warning that should have ended this argument before it started. On March 8, 2023 — two years before the first ByHeart baby got sick — the FDA sent a Call-to-Action letter to every manufacturer, packer, distributor, importer, and retailer of powdered infant formula in the country, signed by the Commissioner of Food and Drugs and the Director of the agency’s food-safety center. It did not bury the issue; it named the organism. The agency wrote that “historical associations between powdered infant formula and pathogens such as Cronobacter spp., Salmonella, and Clostridium botulinum should be considered when designing and implementing controls for the safe manufacture of all foods for infants and young children.” The United States government told this industry, in writing and by genus and species, to control for botulism. Then it watched the industry not do it.
The agency even said it would do more. In March 2025, under its “Operation Stork Speed” initiative, the FDA announced it would increase testing of infant formula and its ingredients for spore-forming contaminants — naming Clostridium botulinum and Bacillus cereus specifically. That announcement came months before the ByHeart outbreak was announced. But announcing that the government will test is not the same as requiring that the hazard be controlled before a single can reaches a shelf.
Everyone with a seat at the table knew the spores were in the milk. They knew the milk wasn’t sterilized. They knew the powder wasn’t sterile. And they decided that because no one had yet proven a baby was poisoned this way, there was nothing to control.
Then ByHeart happened and watch how fast the story changed.
FDA started testing milk powder, nonfat dry milk, and whey for botulism — and its own deputy commissioner for human foods said publicly that the testing would help determine whether this is a “foreseeable hazard that companies could test for.” I had to put the paper down. Yes. It is. It was.
Codex agreed — in December 2025, and only because of ByHeart, the international food-hygiene committee finally opened work on controlling C. botulinum in infant formula. ByHeart, for its part, now promises to test every dairy ingredient and every finished batch for botulism before release.
I will say what I said when the inspection report came out: you do not get credit for installing the smoke detector after the house has burned down.
There is something else worth saying out loud. Both the ByHeart and Nara outbreaks were organic whole milkformulas, and in the ByHeart case FDA genetically matched the botulism in the formula to the organic whole milk powder that went into it. I am not going to stand here and tell you whole milk is the villain. The honest point is narrower, and worse: the safety standards never bothered to ask whether premium, pasture-sourced, whole-milk powder might carry a different spore load than the commodity powder their comfortable assumptions were built on. They assumed low risk across the board, and never checked.
This is the real failure: a regulatory system that treated the absence of proven dead babies as proof of safety. “Causality not yet demonstrated” is a confession dressed up as a finding. It means we are going to keep selling this until a sick baby proves us wrong. Forty-eight babies, and then three more, proved them wrong.
So do better. Specifically:
- Make it mandatory. FDA and Codex should require botulism and clostridial-spore controls and testing for the dairy ingredients that go into infant formula — not “voluntary,” not “consider,” but required, including the sulphite-reducing-clostridia process indicators the experts themselves identified more than a decade ago.
- Finish the work now. Codex opened the file in December. Do not let it die in five years of meetings. Babies do not run on a committee calendar.
- Treat the powder like what it is. Powdered formula is not sterile. Stop letting anyone — regulator or marketer — imply that it is. A parent mixing a bottle for a newborn deserves the truth on the label.
- Open the records. No parent should have to file a FOIA request, and fight through redactions, to learn what a company told the government about the milk in their baby’s bottle. The submissions, the hazard analyses, the inspection findings — put them in the sunlight.
Every one of these cases is a preventable failure that happened before a single baby got sick. The spores were always in the milk. The only question was whether anyone with the power to act would look before, or only after.
They looked after. Again.
Do better.