
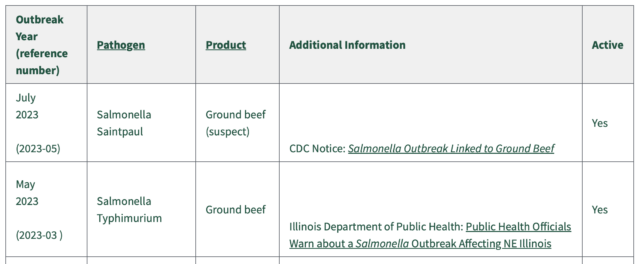
FSIS investigates 2 Mystery Salmonella Outbreaks linked to Ground Beef
It has been a busy July.


C&E Farms Inc., of Oxnard, CA, is recalling certain bins of romaine lettuce because the product may be contaminated with rodent droppings.
According to the details posted online by the FDA, the recall was initiated on June 16, 2023, and is ongoing.
The recalled product was distributed in Massachusetts and Minnesota.
Recalled products:
Anyone who purchased the recalled product should immediately dispose of it and not consume it.
Food products exposed to filth, like rodents, can make you or your family members sick. Rodents can transmit disease through their waste.
Rats and mice carry two main types of disease in their waste: Salmonellosis and Leptospirosis.
I just got this email from a lawyer that I have worked with several times over the years. I hope all lawyers get an email like this once in their practice – mine is pushing 36 years.
Retirement has freed me of the political and financial strains of formal law firm culture, liberating my mind to see the practice, and the practitioners, as they are. I wanted to reach out to you to tell you that in my view you stand out in the crowd for many reasons. First, of course—expertise in your practice. In a sea of posers, you walk the walk. Next—dedication—its is abundantly clear you care deeply about food safety and protecting the public. Finally—ethical compassion——you treat your clients as all lawyers should but most do not—that you are the best in class yet charge a lower percentage fee than you are permitted to says everything about you. You truly do well by doing good.
What is Listeria?
Listeria is a bacterium that causes a serious infection called listeriosis. Around 300 deaths in the United States are caused by Listeria infection each year, according to estimates from a 2011 CDC report.
Listeria bacteria are most found in raw foods. Vegetables can be contaminated by soil and water carrying bacteria. Listeria is also found in raw animal products, such as meat and cheese.
Babies can be born with Listeria if the mother eats contaminated food during pregnancy. The death rate among newborns with Listeria is 25 to 50 percent.
Who is most likely to get seriously ill from Listeria bacteria?
Healthy adults and children hardly ever become seriously ill from Listeria. However, people at increased risk of illness from Listeria bacteria include:
Symptoms of Listeria
Listeria symptoms appear anywhere between 3 and 70 days after infection, but usually around 21 days later. Typical symptoms include:
If infection spreads to the central nervous system, symptoms can include:
Symptoms for those with Weakened Immune Systems
If a patient has a weak immune system, Listeria bacteria can invade the central nervous system and cause meningitis or a brain infection.
Symptoms for Pregnant Women and Newborns
Infected pregnant woman experience mild, flu-like symptoms. However, infection during pregnancy can lead to miscarriage, infection of the newborn, or stillbirth. Symptoms usually appear in newborns in the first week of life but can also occur later on. A newborn’s Listeria symptoms are often subtle, and include irritability, fever, and poor feeding.
Diagnosis of Listeria
Doctors can determine whether patients have listeriosis by taking a blood or spinal fluid sample.
Treatment of Listeria
Patients who present with symptoms of listeriosis can be treated with antibiotics.
How to Prevent Listeria
Foods to Avoid
Additional Resources:
Marler Clark, The Food Safety Law Firm, is the nation’s leading law firm representing victims of Listeria outbreaks. The Listeria lawyers of Marler Clark have represented thousands of victims of Listeria and other foodborne illness outbreaks and have recovered over $850 million for clients. Marler Clark is the only law firm in the nation with a practice focused exclusively on foodborne illness litigation. Our Listeria lawyers have litigated Listeria cases stemming from outbreaks traced to a variety of foods, such as lettuce, polony, deli meat, cantaloupe, cheese, celery and milk.
If you or a family member became ill with a Listeria infection after consuming food and you’re interested in pursuing a legal claim, contact the Marler Clark Listeria attorneys for a free case evaluation.

“Genetic fingerprinting results (whole genome sequencing) indicate that these patients likely have the same source of infection. Patients became ill between February 27 and June 30, 2023.” (Tacoma News Tribune)
Tacoma-Pierce County Department of Health reports that it is working with Washington State Department of Health (DOH) and Thurston County Public Health and Social Services to investigate 5 cases of the foodborne illness listeriosis in Western Washington.
Four of the cases are in Pierce County. One is in Thurston County. All 5 patients were hospitalized and 3 died. All the cases were in patients with weakened immune systems in their 60s or 70s.
Investigators are interviewing patients or their proxies to help identify any common exposures.
Listeriosis is an infection caused by the bacteria Listeria monocytogenes. We see about 10-25 cases in Washington each year. Those most at risk for listeriosis are people who have a weakened immune system or are pregnant, newborn, or elderly. Centers for Disease Control and Prevention (CDC) says it is rare for people outside of these groups to get sick with Listeria infection.
The most common way people get listeriosis is by eating food contaminated with Listeria. Symptoms usually develop between 3-70 days after exposure. About half of those infected see symptoms within 3 weeks.
To protect yourself from listeriosis:
People most at risk of infection should avoid:
Learn more on CDC’s website.
If you think you have a foodborne illness or serious infection, contact your healthcare provider, especially if you are at risk of severe infection.
You can report suspected foodborne illnesses or concerns in Pierce County on our website and in Thurston County here.
DOH is leading this investigation and will continue to update information on its webpage. You can direct media inquiries to doh-pio@doh.wa.gov.
Federal public health officials continue to identify more patients in ongoing outbreaks of foodborne illnesses – E. coli, Salmonella, Cyclospora and Hepatitis A.
In an outbreak of E. coli infections from an unknown source, the patient count has grown to 12, up from 11 a week ago. Investigators have initiated traceback efforts, according to an FDA notice, but the agency has not reported what food or foods are being traced. The FDA has not released any patient information, including where the patients live.
The hepatitis A outbreak increased by one to ten and has been linked to frozen strawberries. The Salmonella outbreak has not been linked to a food product.
For an outbreak of Cyclospora cayetanensis, the case count has increased from 38 to 43 cases in the past week. This incident now includes additional illnesses based on similarities in reported exposures, according to the FDA, however, the agency has not reported what those exposures are. The FDA has initiated onsite inspections and has begun sample collection and analysis, However, the agency has not reported what location is being inspected or what food is being sampled. The FDA has not released any patient information, including where the patients live.
In a separate outbreak of Cyclospora cayetanensis, the case count has increased from 112 to 118 cases. Cyclospora parasites are often associated with various types of fresh produce, including basil, cilantro, mesclun lettuce, raspberries, and snow peas. Food safety experts say washing products does not remove the parasite.
In the third outbreak from the Cyclospora parasite at least 210 people across 22 states have been sickened. Public health officials have not yet determined the source of the parasite.

I have been warning against this since at lease 2005:
See also, www.fair-safety.com
Now from our friends at MMWR:
On June 22, 2022, the Tennessee Department of Health (TDH) was notified of a child hospitalized with Shiga toxin–producing Escherichia coli (STEC) O157:H7 after attending a farming camp at farm A. Three days later, TDH was notified of a second hospitalized child with hemolytic uremic syndrome, whose brother had attended the same camp, prompting an investigation. During the summer, farm A held three week-long summer camps teaching animal husbandry to children aged 6–10 years by assigning campers a baby goat (kid) to care for. STEC resides in the gastrointestinal tract of ruminants such as cattle, goats, sheep, and deer without causing illness in the animal* (1). Outbreaks among humans associated with petting zoos are well documented (2–5).

Investigation and Outcomes
On June 28 and 29, TDH conducted an environmental assessment at farm A. In addition to an onsite interview with the farm owners and employees, the assessment included facility observations of animal pens, public petting areas, areas where children cared for the animals, food service facilities, handwashing and sanitizing facilities, play areas, and toilets. Health department staff members collected camp attendee registration and goat assignment records and conducted environmental sampling, including the collection of 41 samples from animals, animal feces, animal pens, water sources, and toilets.
TDH also sent an online survey to the parents and guardians of all 82 children who had attended camp at farm A during June 6–24 to ascertain dates of attendance, illnesses and outcomes, foods consumed, and camp activities. The outbreak-specific survey was completed by parents or guardians of 53 (65%) campers.
Survey responses facilitated conduct of a case-control analysis. Cases were defined in terms of 1) the person who was ill (primary versus secondary) and 2) the symptoms and laboratory results (probable versus confirmed). A primary case was defined as an illness in a person who attended any of the three camps during June 6–24; a secondary case was a compatible illness within 10 days of exposure to a primary case in the same household or to a close contact of a summer camp attendee (irrespective of illness in the attendee). Probable cases included the onset of diarrhea within 10 days of attending the summer camp (primary cases) or within 10 days of exposure to a secondary case; confirmed outbreak cases were defined as a positive polymerase chain reaction or enzyme immunoassay Shiga toxin test result from a specimen collected after June 6.† Twelve primary cases (including two confirmed and 10 probable) and two secondary cases (one confirmed and one probable) were identified (patient age range = 2–38 years) (Figure). One patient each with a primary and secondary case was hospitalized; one death occurred in a child aged 2 years with a secondary confirmed case.
The case-control analysis included 12 ill camp attendees as case-patients and 58 healthy children identified from the camp attendee list as controls. Chi-square analysis was used to calculate odds ratios; 95% CIs that excluded 1 were considered statistically significant. Because the camp’s food and activity schedules did not change between weeks, and no contributing factors were identified in farm A’s food service establishment, neither a specific activity nor food was considered to be associated with illness. Attendance during the first week of camp, however, was significantly associated with illness (odds ratio = 13.1; 95% CI = 2.59–66.57). Camp operators reported being aware of the National Association of State Public Health Veterinarians Animal Contact Compendium§ and reported incorporating handwashing stations, observing children during animal interactions, and keeping the animal areas clean and disinfected.
Investigators were able to isolate STEC by culture in six samples collected at farm A; these were further subtyped into three STEC serotypes by core genome multilocus sequence typing: H14 (one rectal swab [kid] and one stool swab [kid]), O157:H7 (one stool swab [kid] and one wood swab [inside kid barn]), and O26:H11 (two stool samples [kids]).¶ Only STEC O157:H7 was associated with clinical illnesses. The two farm A STEC O157:H7 isolates were closely related by whole genome sequencing to the three outbreak-associated STEC O157:H7 patient isolates.
Preliminary Conclusions and Actions
In response to the outbreak, farm A voluntarily closed the camp, expedited the demolition of the kid barn, euthanized two kids with positive STEC test results, and moved the kid herd off the property. During closure, farm A independently consulted with veterinarians and other petting zoos to identify additional methods for reducing disease transmission. Based on recommendations provided, the facility discontinued the animal husbandry portion of the camp, increased signage encouraging handwashing after touching animals or objects throughout the facility, and increased messaging on their website about zoonotic diseases, populations at highest risk, and ways to mitigate risk for infection. On July 18, farm A reopened their summer camp without the goat husbandry component.
TDH concluded that this outbreak was associated with STEC O157:H7-infected kids and involved secondary transmission. Hand-to-mouth contact has been observed to occur almost three times per hour among children aged 6–10 years,** supporting the potential for STEC ingestion from contaminated environmental surfaces. The hypothesis of prolonged contact between campers and kids resulting in illness is strengthened by the finding that, after conducting routine monitoring of pathogen and case report forms as well as complaint surveillance systems, STEC was not identified by patrons of the farm apart from camp attendees and their household members. Animal farms, petting zoos, and other environments where small children might have direct contact with ruminant animals should be aware of the risk for zoonotic STEC transmission and make efforts to mitigate these risks by promoting proper hand hygiene during and after animal contact.
Acknowledgments
Tennessee Department of Health Communicable and Environmental Diseases and Emergency Preparedness Food Outbreak Team; Tennessee Department of Health Public Health Laboratory Team; Tennessee Department of Health Environmental Health Team; Nathan Miller, Mark Morgan, University of Tennessee Agricultural Extension; Eric Coffey, Tennessee Department of Health Southeast Regional Office; Mary-Margaret Fill, Tennessee Department of Health.
References


Ten people in Washington, Oregon, California and Hawaii have contracted Hepatitis A linked to the consumption of frozen strawberries. Epidemiologic and traceback evidence indicate that frozen organic strawberries, imported fresh from certain farms located in Baja California, Mexico in 2022, are the source of this outbreak. The hepatitis A virus strain causing illnesses in this outbreak is genetically identical to the strain that caused a foodborne hepatitis A outbreak in 2022, which was linked to fresh organic strawberries imported from Baja California, Mexico, and sold at various retailers.
In response to this investigation, California Splendor, Inc. of San Diego, California voluntarily recalled certain lots of 4-lb. bags of Kirkland Signature Frozen Organic Whole Strawberries that were sold at Costco stores in Los Angeles, California; Hawaii; and two San Diego, California business centers. The lots subject to this recall include: 140962-08, 142222-23, 142792-54, 142862-57, 142912-59, 142162-20, 142202-21, 142782-53, 142852-56, 142902-58, 142212-22, 142232-24, 142842-55. In response to this investigation, Scenic Fruit Company of Gresham, Oregon voluntarily recalled frozen organic strawberries, sold to Costco, Trader Joe’s, Aldi, KeHE, Vital Choice Seafood, and PCC Community Markets in certain states.
Other products subject to this recall include:
What you need to know.
During the COVID-19 Pandemic (it really is not over yet), foodborne illness outbreaks were down, and I said a few days ago, they are back – CDC Report: We are back to “Bad Normal” with foodborne illnesses as COVID wanes. Well, if the recent rash of norovirus outbreaks on cruise ships is any indication, norovirus and cruise ships are also back. Here is the lates from the CDC:

The Centers for Disease Control and Prevention (CDC) estimates that noroviruses cause nearly 21 million cases of acute gastroenteritis annually, making noroviruses the leading cause of gastroenteritis in adults in the United States. Of the viruses, only the common cold is reported more often than a norovirus infection—also referred to as viral gastroenteritis.
Humans are the only host of norovirus. Norovirus causes nearly 60% of all foodborne illness outbreaks. Norovirus is transmitted primarily through the fecal-oral route, with fewer than 100 norovirus particles needed to cause infection. Moreover, the viruses can spread quickly, especially in places where people are in proximity, such as cruise ships and airline flights, even those of short duration. Common settings for norovirus outbreaks include restaurants and events with catered meals (36%), nursing homes (23%), schools (13%), and vacation settings or cruise ships (10%).
Outbreaks of norovirus infections have become synonymous with cruise ships. Healthcare facilities also experience a high incidence of norovirus outbreaks. The CDC has published information regarding the prevention of norovirus outbreaks on cruise ships and in healthcare facilities on its website. Once a case has occurred, even more stringent hygienic measures than normal are required to prevent an outbreak, particularly on an enclosed space such as a cruise ship.
Norovirus illness usually develops 24 to 48 hours after ingestion of contaminated food or water. Symptoms typically last a relatively short amount of time, approximately 24 to 48 hours. Symptoms of norovirus include nausea, vomiting, diarrhea, and abdominal pain. Headache and low-grade fever may also accompany this illness. People infected with norovirus usually recover in two to three days without serious or long-term health effects.
Although symptoms usually only last one to two days in healthy individuals, norovirus infection can become quite serious in children, the elderly, and immune-compromised individuals. In some cases, severe dehydration, malnutrition, and even death can result from norovirus infection, especially among children and among older and immune-compromised adults in hospitals and nursing homes. Recently, there have been reports of some long-term effects associated with norovirus, including necrotizing entercolitis, chronic diarrhea, and post-infectious irritable bowel syndrome.
References
1. American Public Health Association (APHA), Heymann, David L., editor, “Norovirus Infection,” in CONTROL OF COMMUNICABLE DISEASES MANUAL, pp. 227-29, (18th Ed. 2008).
2. Antonio, J, et al., “Passenger Behaviors During Norovirus Outbreaks on Cruise Ships,” INTERNATIONAL SOCIETY OF TRAVEL MAGAZINE, Vol. 15, No. 3, pp. 172-176 (May-June 2008). Abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/18494694
3. Benson, V. and Merano, M.A., “Current estimates from the National Health Interview Survey 1995,” VITAL HEALTH STATISTICS, SERIES 10 (Nat’l Center for Health Statistics 1998). Abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/9914773
4. Cáceres, VM, et al., “A viral gastroenteritis outbreak associated with person-to-person spread among hospital staff,” INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY, Vol. 19, No. 3, pp. 162-7 (March 1998). Abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/9552183
5. CDC, Norovirus: Technical Fact Sheet, from Centers for Disease Control and Prevention Web site, http://www.cdc.gov/ncidod/dvrd/revb/gastro/norovirus-factsheet.htm (last modified on August 24, 2011) (last checked on Jan. 3, 2012).
6. CDC, Norovirus in Healthcare Facilities Fact Sheet, available through Centers for Disease Control and Prevention website, at http://www.cdc.gov/hai/pdfs/norovirus/229110-ANoroCaseFactSheet508.pdf (last checked on January 4, 2012).
7. CDC, Facts about Norovirus on Cruise Ships, last updated July 20, 2009, available through the Centers for Disease Control and Prevention website, at http://www.cdc.gov/nceh/vsp/pub/Norovirus/Norovirus.htm (last checked on January 4, 2012).
8. CDC, “Outbreaks of Gastroenteritis Associated with Noroviruses on Cruise Ships – United States, 2002,” MORBIDITY AND MORTALITY WEEKLY REPORT, Vol. 51, No. 49, pp. 1112-15 (Dec. 13, 2002). Full text available online at http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5149a2.htm
9. CDC, “Updated Norovirus Outbreak Management and Disease Prevention Guidelines,” MORBIDITY AND MORTALITY WEEKLY REPORT, Vol. 60, Recommendations and Reports No. 3, pp. 1-15 (March 4, 2011). Full text available online at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6003a1.htm
10. CDC, “Norwalk-like viruses’—Public health consequences and outbreak management,” MORBIDITY AND MORTALITY WEEKLY REPORT, Vol. 50, Recommendations and Reports No. 9, pp. 1-18 (June 1, 2001). Full text available online at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5009a1.htm
11. Duizer, E, et al., “Probabilities in norovirus outbreak diagnosis,” JOURNAL OF CLINICAL VIROLOGY, Vol. 40, No. 1, pp. 38-42 (Sept. 2007). Abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/17631044
12. Donaldson, E., et al., “Viral shape-shifting: norovirus evasion of the human immune system,” NATURE REVIEWS, MICROBIOLOGY, Vol. 8, No. 3, pp. 231-239 (March 2010). Abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/20125087
13. Fankhauser, RL, et al., “Epidemiologic and molecular trends of ‘Norwalk-like viruses’ associated with outbreaks of gastroenteritis in the United States,” JOURNAL OF INFECTIOUS DISEASES, Vol.186, No. 1, pp. 1-7 (July 1, 2002). Full text of article available online at http://jid.oxfordjournals.org/content/186/1/1.long
14. Gerencher, Christine L., Reporter, “Understanding How Disease Is Transmitted via Air Travel: Summary of a Symposium,” Conference Proceedings 47, Transportation Research Board of the National Academies (2010). Full summary available online at http://onlinepubs.trb.org/onlinepubs/conf/CP47.pdf
15. Glass, RI, et al., “The Epidemiology of Enteric Caliciviruses from Humans: A Reassessment Using New Diagnostics,” JOURNAL OF INFECTIOUS DISEASES, Vol. 181, Supplement 2, pp. S254-61 (2000). Full text available online at http://jid.oxfordjournals.org/content/181/Supplement_2/S254.long
16. Glass, R, Parashar, U.D., and Estes, M.K., “Norovirus Gastroenteritis,” NEW ENGLAND JOURNAL OF MEDICINE, Vol. 361, No. 18, pp. 1776-1785 (Oct. 29, 2009). Full text available online at http://www.sepeap.org/archivos/pdf/11191.pdf
17. Janneke, C, et al., “Enhanced Hygiene Measures and Norovirus Transmission during an Outbreak,” EMERGING INFECTIOUS DISEASES, Vol. 15, No., pp. 24-30 (Jan. 2009). Full text available online at http://wwwnc.cdc.gov/eid/article/15/1/08-0299_article.htm
18. Harris, JP, et al., “Deaths from Norovirus among the Elderly, England and Wales,” EMERGING INFECTIOUS DISEASES, Vol. 14, No. 10, pp. 1548-1552 (Oct. 2008). Full text available online at http://wwwnc.cdc.gov/eid/article/14/10/08-0188_article.htm
19. Kirkland, KB, et al., “Steaming oysters does not prevent Norwalk-like gastroenteritis,” PUBLIC HEALTH REPORTS, Vol. 111, pp. 527-30 (1996). Full text available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1381901/pdf/pubhealthrep00045-0057.pdf
20. Maunula, L, Miettinen, IT, and Bonsdorff, CH, “Norovirus Outbreaks from Drinking Water,” EMERGING INFECTIOUS DISEASES, Vol. 11, No. 11, pp. 1716-1721 (2005). Full text available online at http://wwwnc.cdc.gov/eid/content/11/11/pdfs/v11-n11.pdf
21. Lopman, Ben, Zambon, Maria, and Brown, David, “The Evolution of Norovirus, the ‘Gastric Flu,’” Public Library of Science: Medicine, Vol. 5, Issue 2, pp.187-189 (Feb. 2010). Full text available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2235896/pdf/pmed.0050042.pdf
22. Lowther, J, Henshilwood, K, and Lees DN, “Determination of Norovirus Contamination in Oysters from Two Commercial Harvesting Areas over an Extended Period, Using Semiquantitative Real-Time Reverse Transcription PCR,” JOURNAL OF FOOD PROTECTION, Vol. 71, No. 7, pp. 1427-1433 (2008). Abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/18680943
23. Lysen, M, et al., “Genetic Diversity among Food-Borne and Waterborne Norovirus Strains Causing Outbreaks in Sweden,” JOURNAL OF CLINICAL MICROBIOLOGY, Vol. 47, No. 8, pp. 2411-2418 (2009). Full text available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2725682/?tool=pubmed
24. Marks, PJ, et al., “Evidence of airborne transmission of Norwalk-like virus (NLV) in a hotel restaurant,” EPIDEMIOLOGY AND INFECTION, Vol. 124, No. 3, pp. 481-87 (June 2000). Full text available online at http://www.cdc.gov/nceh/ehs/Docs/Evidence_for_Airborne_Transmission_of_Norwalk-like_Virus.pdf
25. Mayo Clinic, “Norovirus Infection,” Mayo Clinic Web site, information last updated April 15, 2011 (as of last checking on Jan. 3, 2012), available online at http://www.mayoclinic.com/health/norovirus/DS00942/DSECTION=1
26. Mead, Paul M, et al., “Food-related Illness and Death in the United States,” EMERGING INFECTIOUS DISEASES, Vol. 5, No. 5, pp. 607-25 (September-October 1999). Full text available online athttp://www.ncbi.nlm.nih.gov/pmc/articles/PMC2627714/pdf/10511517.pdf
27. Middleton, PJ, Szmanski, MT, and Petric M, “Viruses associated with acute gastroenteritis in young children,” AMERICAN JOURNAL OF DISEASES OF CHILDREN, Vol. 131, No. 7, pp. 733-37 (July 1977). Abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/195461
28. Patterson, T, Hutchin, P, and Palmer S, “Outbreak of SRSV gastroenteritis at an international conference traced to food handled by a post symptomatic caterer,” EPIDEMIOLOGY AND INFECTION, Vol. 111, No. 1, pp. 157-162 (Aug. 1993). Available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2271183/?tool=pubmed
29. Ozawa, K, et al., “Norovirus Infections in Symptomatic and Asymptomatic Food Handlers in Japan,” JOURNAL OF CLINICAL MICROBIOLOGY, Vol. 45, No. 12, pp. 3996-4005 (Oct. 2007). Abstract available online at http://jcm.asm.org/content/45/12/3996.abstract
30. Said, Maria, Perl, Trish, and Sears Cynthia, “Gastrointestinal Flu: Norovirus in Health Care and Long-Term Care Facilities,” HEALTHCARE EPIDEMIOLOGY, vol. 47, pp. 1202-1208 (Nov. 1, 2008). Full text available online at http://cid.oxfordjournals.org/content/47/9/1202.full.pdf+html
31. Scallan, E., et al., “Foodborne Illness Acquired in the United States—Major Pathogens,” EMERGING INFECTIOUS DISEASES, Vol. 17, No. 1, pp. 7-15 (2011). Full text available online at http://wwwnc.cdc.gov/eid/article/17/1/p1-1101_article.htm
32. Siebenga, JJ, et al., “Norovirus Illness Is a Global Problem: Emergence and Spread of Norovirus GII.4 Variants, 2001–2007,” JOURNAL OF INFECTIOUS DISEASES, Vol. 200, No. 5, pp. 802-812 (2009). Full text available online at http://jid.oxfordjournals.org/content/200/5/802.long
33. Treanor, John J. and Dolin, Raphael, “Norwalk Virus and Other Calciviruses,” in Mandell, Douglas, and Bennett’s PRINCIPLES AND PRACTICE OF INFECTIOUS DISEASES, Fifth Edition, Chap. 163, pp. 1949-56 (2000, Mandell, Bennett, and Dolan, Editors).
34. Tu, E.T., et al., “Epidemics of Gastroenteritis during 2006 Were Associated with the Spread of Norovirus GII.4 Variants 2006a and 2006b,” CLINICAL INFECTIOUS DISEASES, Vol. 46, No. 3, pp. 413-420 (Feb. 1, 2008). Full text available online at http://cid.oxfordjournals.org/content/46/3/413.full
35. Tu E.T., et al., “Norovirus excretion in an age-care setting,” JOURNAL OF CLINICAL MICROBIOLOGY, Vol. 46, pp. 2119-21 (June 2008). Full text available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2446857/pdf/2198-07.pdf
36. Verhoef, L, et al., “Emergence of New Norovirus Variants on Spring Cruise Ships and Prediction of Winter Epidemics,” EMERGING INFECTIOUS DISEASES, Vol. 14, No. 2, pp. 238-243 (Feb. 2008). Full text available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2600213/pdf/06-1567_finalR.pdf
37. Vinje, J, “A Norovirus Vaccine on the Horizon?” EMERGING INFECTIOUS DISEASES, Vol. 202, No. 11, pp. 1623-1625 (2010). Full text available online at http://jid.oxfordjournals.org/content/202/11/1623.full
38. Westrell T, et al., “Norovirus outbreaks linked to oyster consumption in the United Kingdom, Norway, France, Sweden and Denmark,” EURO-SURVEILLANCE (European Communicable Disease Bulletin), Vol. 15, No. 12 (Mar. 25 2010). Full text available online at http://www.eurosurveillance.org/images/dynamic/EE/V15N12/art19524.pdf