
Lawrence J. O’Connor is a 70-year-old gentleman residing in Beresford, South Dakota with his wife Ruth. Lawrence and Ruth were visiting his daughter in Phoenix, Arizona for a few weeks when they decided to go out for dinner. On Friday, March 23, 2018, the two went to dinner at Red Lobster located at 7921 W. Bell Rd. in Peoria, Arizona 85382. Lawrence chose a Caesar salad made with romaine lettuce, and his wife and a regular salad.

Lawrence and Ruth in February 2018
Symptom Onset
Over the next 24-48 hours after Lawrence and his wife dined at Red Lobster, he began to get sick. He first had stomaching cramping and diarrhea on Monday, March 26, 2018. The diarrhea continued to get worse and he noticed there was blood in it on Tuesday. By the following day, there was so much blood he could no longer pass it off as hemorrhoids or something insignificant, and he decided to seek medical care.
Banner Thunderbird Medical Center
Just before 9 PM on Wednesday, March 28, 2018, Lawrence presented to Banner Thunderbird Medical Center, where Jody Boyer, PA evaluated him in the emergency department under the supervision of Kristen Niedner, MD. In triage, Lawrence described have abdominal pain and diarrhea since Monday, March 26, which had become bloody the morning of the 28th. He had experienced three bloody stools since then and decided to seek medical attention in the ER. He described his abdominal pain as non-focal, and his stool were previously watery. He had vomited once. Lawrence described that it was the bright red blood in his diarrhea that caught his attention and caused him great alarm, leading to the ER visit. He answered questions about possible exposures to suspect food or others who were sick, and he stated he had not been out of the country, had not taken any recent antibiotics, and had not eaten any food he thought was bad. He indicated he had not been around others with similar symptoms.
On exam, PA Boyer found Lawrence afebrile with unremarkable vital signs. She confirmed diffuse abdominal pain and stool positive for occult blood by guaiac testing. His abdomen was soft and non-distended, without guarding or rebound tenderness. The PA sent blood and urine samples to the lab, which returned results showing an elevated white blood cell count of 15.4.[1]
CT scan – mild acute colitis
At 11:50 PM, radiologist Raul Galvez-Trevino, MD performed a contrast-enhanced CT scan of Lawrence’s abdomen and pelvis, during which he identified mild acute colitis involving the ascending and transverse colon, suspicious for either an infectious or inflammatory etiology. He also observed possible mild right pyelitis (kidney inflammation) that he thought warranted further investigation. The PA conferred with the attending physician, who concurred with a clinical impression of “acute diffuse abdominal pain,” “acute rectal bleeding,” “acute ascending and transverse colon colitis,” and “possible mild right pyelitis,” noting his co-morbidities of hypertension history, coronary artery disease, arthritis, and hyperlipidemia.
While he was under observation in the ER, Lawrence was started on intravenous fluids and IV antibiotics (Levaquin 750 mg and metronidazole 500 mg), and a recheck of his anemia by CBC revealed a stable blood count. The hospitalist service was consulted and the decision was made to admit Lawrence for observation, at least overnight.
Arun Pillai, MD came in for an urgent gastroenterology consultation while Lawrence was still in the ER and reviewed the CT results with radiology. Dr. Pillai thought that Lawrence had a lower gastrointestinal bleed related to his right-sided colitis. He was not sure of the cause but was most suspicious for an infectious etiology and less likely an inflammatory etiology. He opined that ischemia was unlikely, based on the distribution of colitis seen on CT. Dr. Pillai observed that Lawrence’s initial stool results were back, showing negative for toxigenic C. difficile.
Admission to hospital
It was after midnight on March 29, 2018 by the time Sanjay Kulkarni, MD formally admitted Lawrence to the hospital for abdominal pain and rectal bleeding. He noted that Lawrence had a medical history that was significant for coronary artery disease (“status post 4-vessel CABG”), hypertension, and hyperlipidemia. He repeated his history and physical exam, and Lawrence reiterated that he started to have diarrhea 2 to 3 days prior to admission. “This was with almost every time he ate.” Lawrence also reported having fevers and chills at home. He stated he took a full-strength aspirin tablet (325 mg) every day but was not on any other blood thinners. He reported his abdominal pain level as severe, or about 8/10 on a 1-10 pain scale. Lawrence reported a previous colonoscopy 8 years earlier in South Dakota and was told it was normal. Dr. Kulkarni noted that Lawrence had not been tachycardic or hypotensive in the ER. He admitted Lawrence on telemetry observation and continued his IV antibiotics.
Hospital Day 2 – discharged home
On March 30, 2018, hospitalist Karen Alonzo, MD evaluated Lawrence for discharge from the hospital. She reviewed his blood work and deemed him clinically stable and appropriate for continued self-care at home. She provided a written prescription to continue taking Levaquin and Flagyl in oral form to complete a ten-day course, as well as Zofran for nausea and Percocet for pain. She advised him to follow-up with his PCP and gastroenterology as an outpatient. His stool studies were still pending at the time he was discharged home.
Confirmation of stool-positive Shiga toxin 2
After Lawrence had already been discharged from the hospital, at 8:48 PM the Banner Hospital laboratory reported a critical value that his stool had tested positive for Shiga toxin 2. The lab report carried the warning: “Positive Shiga-toxin results are most commonly due to Shiga-toxin producing E. coli (O157 or non O157 STEC) which may cause enterohemorrhagic disease and Hemolytic Uremic Syndrome (HUS). Antimicrobial therapy is not required unless the corresponding stool culture is also positive for Shigella.”[2]
On March 31, 2018, the Banner Hospital Laboratory reported that Lawrence’s stool culture was negative for growth of Salmonella, Shigella, and Campylobacter.
Home but not better…
Lawrence recalls: “[The hospital] gave me pills to take and sent me home on Friday. I still had bloody diarrhea. On the Monday after Easter, I got up and passed out enough to fall. My wife called the ambulance and they came and checked me out and I passed out again. They then took me to a different hospital as for what was wrong a different one was better.”
Phoenix Fire Department
On Tuesday, April 2, 2018 around 8 AM, EMS responded to a call from Lawrence’s family that he had an episode of dizziness and almost fainted. Upon their arrival at the family residence, the first responders found Lawrence sitting, alert, and oriented. He stated that he was not having any chest pain, difficulty breathing, or loss of consciousness, and he had not become diaphoretic before the near-syncopal event. They transported him via ALS ambulance transport to the hospital.
Honor Health – Deer Valley Hospital
Lawrence arrived at Deer Valley Hospital around 9 AM on April 2, 2018, where Michael Saam Karbasi, MD evaluated him in the emergency department. Dr. Karbasi observed that Lawrence had just been discharged from Thunderbird on Friday, March 29, where he had been kept overnight for colitis and rectal bleeding. Lawrence reported that he began feeling dizzy while in the shower the night of the 30th before falling down that morning. The near-syncopal episode had been witnessed by his wife.
According to the EMS report, Lawrence’s initial blood pressure at the family residence was 66/42, but after a 500 cc bolus of IV fluids, it improved to 82/46. Lawrence had his hospital records with him from Thunderbird, with the CT scan result that showed mild acute colitis. He stated that he had been taking his antibiotics as prescribed since he was discharged home three days earlier, and his diarrhea had started to improve; however, he continued to have persistent rectal bleeding, although the amount was small and his stool was beginning to return to normal color. Lawrence also mentioned that he had a poor appetite and was not hydrating well since going home, although he had not had any more fevers, and no sore throat, cough, nausea, vomiting, urinary complaints, abdominal pain, shortness of breath, or chest pain. He complained of no other symptoms at that time.
Dr. Karbasi restarted Lawrence on IV fluids and send blood to the lab, which returned results showing he still had significant leukocytosis and now exhibited severe anemia and thrombocytopenia, as well as acute renal failure (WBC 25.9, hemoglobin 9.6, platelet count 95K, BUN 94, serum creatinine 7.5). A 12 lead EKG was obtained that showed “sinus bradycardia with 1st degree AV block, rate 59, no ST or T wave elevations or depressions.”
Consultation advises hospital admission
At 11:47 AM, Dr. Karbasi consulted with Shannan Murphy, MD of hospitalist service, who agreed to admit Lawrence to the hospital telemetry unit. She, in turn, requested a nephrology consultation and additional lab tests for clotting abnormalities, as well as insertion of a Foley catheter into his bladder so his fluid balance could be carefully monitored. Dr. Karbasi also consulted with infectious disease about Lawrence’s lab results, after which he immediately stopped Lawrence’s antibiotics, concerned about the risk for hemolytic uremic syndrome, given his anemia, thrombocytopenia, and renal failure. He also requested a stat CT scan.
CT shows colitis and other abnormalities
Tamim Sultani, MD performed an unenhanced CT scan of Lawrence’s abdomen and pelvis, during which he identified extensive colon wall thickening, for which the main differential considerations included infectious/inflammatory colitis or ischemic colitis. In addition, he observed bilateral kidney stones but particularly in the right renal pelvis, as well as gallstones and cirrhosis[3] of Lawrence’s liver. He also observed a small amount of ascites and a small right pleural effusion.
Nephrology Consultation – Possible HUS
Around 2 PM, Guneet Mumick, MD came in for a nephrology consultation and noted that Lawrence’s stool had tested positive for Shiga toxin 2. He reviewed his abnormal renal function labs and told Lawrence and his wife that his acute renal failure was probably secondary to hemolytic uremic syndrome. He told him about the positive Shiga toxin result according to the Banner/Thunderbird records. Lawrence also exhibited low blood sodium, metabolic acidosis, and lower extremity swelling. They discussed the implications of HUS, as well as the possibility of acute tubular necrosis (ATN) from low blood pressure versus acute interstitial nephritis (AIN) from having taken Levaquin. He continued Lawrence’s intravenous fluids, adding oral bicarbonate to his medications. Finally, he discussed that he was going to need hemodialysis as soon as the next day, if his abnormal renal function did not turn around on his lab results. Dr. Mumick added a peripheral blood smear and a haptoglobin level to his blood tests, as well as checking an ADAMTS13 test. They discussed the use of Eculizumab (Soliris) for infectious HUS if there was central nervous system involvement, but he wanted to hold off for now. He planned to monitor his fluid intake and output carefully via IV management and Foley catheter urine measurements
Infectious Disease Consultation
At 4:55 PM, Walid Almut, MD came in for infectious disease at the request of Dr. Murphy. She requested that he consult regarding Lawrence’s “Shiga toxin positive E. coli HUS.” Dr. Almut observed that a stool culture had not been finalized at Thunderbird that confirmed E. coli, although he suspected it was the likely diagnosis. He noted that Lawrence was clinically worse after being given Levaquin and Flagyl, “… which is also more suggestive of Shiga toxin E. coli strain.” Dr. Almut saw that Lawrence had tested negative for toxigenic C. difficile. He emphasized that all antibiotics should be avoided entirely, and Lawrence’s treatment should consist of supportive care only, with IV fluids and albumin. Lawrence was currently afebrile and his blood pressure was improved after receiving additional IV fluid boluses. Dr. Almut requested blood tests for CRP and procalcitonin.
Hematology Consultation – no convincing evidence for HUS
Mazen Khattab MD came in for a hematology consultation at 5:47 PM regarding Lawrence’s anemia and thrombocytopenia. Lawrence reported that he was still having rectal bleeding, and that morning he had experienced a syncopal episode and was found to have anemia and thrombocytopenia with renal failure. Dr. Khattab observed that Lawrence’s hemoglobin that day was low at 9.6, as were his platelets at 85K.
Dr. Khattab reviewed a chest x-ray taken at 4 PM, comparing it to a Nuclear Lung Scan to rule out a pulmonary embolism. Radiologist Jimmy Saade, MD’s chest x-ray impression was that Lawrence had COPD, with “blunting of both costophrenic angles, consistent with small volume pleural effusions versus pleural thickening.” On the Nuclear Medicine V/P scan, there were no observable abnormal matched or mismatched ventilation or perfusion defects. Barry Sadegi, MD observed a symmetric, bilateral distribution of radiopharmaceutical medium on both the perfusion and ventilation images, indicating a negative test result for pulmonary arterial embolism.
Finally, Dr. Khattab personally reviewed Lawrence’s peripheral blood smear. There were rare schistocytes[4], “… but not convincing for MAHA[5] (HUS).” He noted that his LDH was elevated (>300), but his haptoglobin was normal. He commented: The anemia and thrombocytopenia could be from bleeding and acute inflammation and not necessarily from MAHA, especially given the lack of convincing significant schistocytosis on peripheral blood smear. He wanted to monitor Lawrence’s LDH and haptoglobin[6] and peripheral blood smear over the next 24-48 hours before making a final determination.
Hospital Day 2 – Hemodialysis No. 1
On April 3, 2018, Dr. Murphy came in for the hospitalist service during morning rounds and observed that Lawrence had become oliguric[7], with a urinary output of less than 200 cc overnight. His hemoglobin had fallen to 8.8, down from 9.6 gm/dL the day before. His white count was still markedly elevated at 24.5. His BUN and creatinine were 94 and 7.5. A urine culture was pending. Dr. Murphy consulted with nephrology, who made the decision to start Lawrence on hemodialysis that day. Dr. Murphy put in an order for the insertion of a hemodialysis catheter, with the first HD treatment to be initiated afterward.
Hematologist Dr. Khattab came in at 9 AM, and Lawrence told him his rectal bleeding was slowing down and his diarrhea was improving. Dr. Khattab reviewed his labs, noting that his LDH was going down and his haptoglobin was normal. He commented in his chart note:
This argues against ongoing hemolysis. The anemia and thrombocytopenia could be from bleeding and acute inflammation and not necessarily from MAHA, especially given the lack of convincing significant schistocytosis on peripheral blood smear. In fact, platelets are improved today. I will monitor LDH and haptoglobin. At this point, I would monitor conservatively. No convincing evidence of MAHA at this point to justify plasma exchange. Patient is going for HD per Dr. Mumick. Discussed with Dr. Murphy and Dr. Mumick.
Guarav Patel, MD performed the insertion of a right internal jugular temporary hemodialysis catheter later that morning, which was done under fluoroscopy with a right neck entry and selection of a 21 gauge, 5 Fr. dual-lumen catheter. Both lumens were easily aspirated and flushed, and a subsequent chest x-ray confirmed the correct placement with the tip in the superior vena cava. Immediately after HD catheter insertion, Miguel Gonzalez, RN initiated HD under the supervision and direction of the nephrology service, Lixian Zou, MD. Lawrence tolerated the procedure well and was transported back to his room in stable condition after the procedure. His next hemodialysis was scheduled for the 5th.
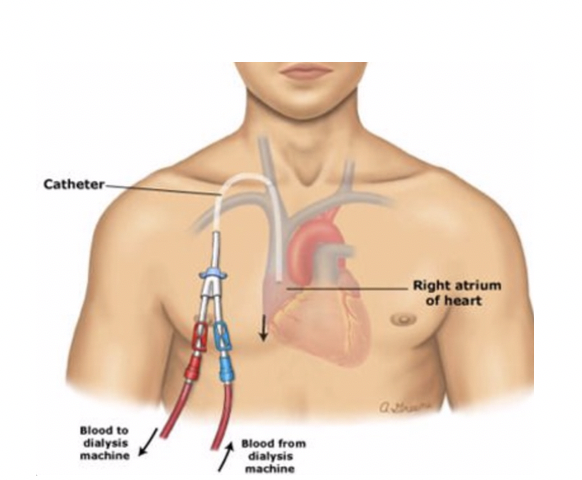
HD catheter insertion
Lawrence was visited by the various specialists on the 3rd and no other changes were made to his care plan. He remained afebrile with stable blood pressures and was beginning to feel better.
Hospital Day 3 – Hemodialysis No. 2 – anuria and altered mental status
On April 4, 2018, Lawrence continued to have diarrhea, although it was no longer bloody. He was now producing almost no urine and was having swelling in both lower extremities. Doppler studies failed to demonstrate any blood clots in the deep veins of his legs. Dr. Katthad continued to trend Lawrence’s lab results, noting a continued decline in his LDH level and a return of his platelets to normal range, and his haptoglobin and peripheral smear were unremarkable. However, Dr. Zou observed that he was effectively anuric with only a 100 ml urinary output in 24 hours, despite of a 5-liter positive fluid balance (3820 input, 2420 output, accounting for fluid removal in dialysis as well as urinary output). His renal function remained markedly abnormal, with a BUN and creatinine of 71 and 7.9.
Dr. Zou discussed doing a renal biopsy to assist with diagnosing the cause for his renal failure, and Lawrence agreed to the procedure and it was scheduled for the 5th. His urine culture was not growing any bacteria thus far. Although hemodialysis had been planned to skip a day and resume on the 5th, Dr. Zou ordered a second session that morning given his worsening renal status.
Dr. Murphy came in for the hospitalist service around midday and was concerned to hear that Lawrence was having hallucinations. He reported seeing things in his room like a hair net and seeing water on the floor when there was none. His blood pressure was doing better and was currently 113/58. He continued to receive albumin in his IV fluids to combat a tendency for hypotension. Dr. Murphy discussed Lawrence’s altered mental status with him and his wife at the bedside, with a plan to consult psychiatry. She was less concerned that his white count was still elevated at 22.9 as he remained afebrile. He was tolerating a renal diet.
Hospital Day 4 – Hemodialysis No. 3 – Renal biopsy
On April 5, 2018, Lawrence’s renal function was no better, with only 120 ml of urinary output in 24 hours, although his serum creatinine was improved at 6.8. What little urine he was producing was significant for a large amount of protein, bilirubin, and leukocyte esterase. His white count remained elevated at 20.3. His liver enzymes were slightly elevated over the prior few days, but a viral hepatitis screen was negative. Another hemodialysis session was implemented that afternoon.
Dr. Murphy came in for the hospitalist service and noted that Lawrence had continued to exhibit confusion during the night. He was better at the time of her visit, but the nurses remarked he had been “quite agitated” overnight. He was alert and oriented to Dr. Murphy’s exam but wanted to know when he could leave the hospital. She ordered an atypical antipsychotic drug (risperdone[8]) for his agitation while a psychiatry consultation was pending.
In the early afternoon, William Romano, MD took Lawrence for a CT guided left-renal cortical core biopsy, which was satisfactorily performed using conscious sedation. The biopsy samples were sent to surgical pathology for analysis. Later in the evening, Kimberly M. Nelson, PA came in for a psychiatry consultation regarding Lawrence’s altered mental status, with confusion and hallucinations. He was doing better that day, but she continued him on the medication started by Dr. Murphy, adding Ambien to be used as needed if he had trouble sleeping. She planned to visit Lawrence daily and remained available for consultation.
Hospital Day 5
On April 6, 2018, Dr. Khattab came in for hematology and reviewed Lawrence’s morning labs, noting that his LDH continued to go down and his haptoglobin was normal. “This argues against ongoing hemolysis.” He again opined that Lawrence’s anemia and thrombocytopenia could be from bleeding and acute inflammation and not necessarily from MAHA, especially given the lack of convincing significant schistocytosis on his peripheral blood smear. His platelets continued to be in normal range. His hemoglobin was slowly worsening since the 4th (8.3à7.9), but his white count had been slowly improving during that time (22.9à20.8).
Dr. Mumick came in for nephrology during the afternoon and observed that Lawrence was still oliguric, but he deferred hemodialysis that day. He considered Lawrence’s hemoglobin “relatively stable,” but his BUN and creatinine remained significantly abnormal at 32 and 5.5, although that was improved from the 5th (49 and 6.8). Lawrence’s renal biopsy results were still pending, as were his results for ADAMTS13[9] testing.
Hospital Day 6-8 – Hemodialysis No. 4 and 5
On April 7, 2018, Lawrence underwent his fourth hemodialysis treatment. He was still oliguric, but Dr. Mumick approved the removal of his Foley catheter, as he was clinically stable. Dr. Mumick gave Lawrence a break from hemodialysis on April 8 and resumed it on the 9th, potentially planning the next session for the 11th. On April 9, 2018, Lawrence’s white count was almost down to normal range, and his anemia remained stable.
Hospital Day 9-10 – Renal biopsy shows post-infectious glomerulonephritis
On April 10, 2018, surgical pathologist Ekaterina Castano, MD called and discussed Lawrence’s renal biopsy results with nephrologist Sachin N. Desai, MD and give him on preliminary report, explaining the findings were suggestive of post-infectious glomerulonephritis. There was no indication of acute tubular necrosis. Dr. Desai reviewed Lawrence’s labs the next morning of April 11, 2018, which showed a worsening of his creatinine level, but his urinary output had begun to increase. He had some lower extremity swelling suggestive of fluid overload, but he had no chest pain or shortness of breath. Dr. Desai did not think Lawrence needed hemodialysis that day.
Hospital Day 11-12 – Discharged. home
On April 12, 2018, Dr. Desai came back to see Lawrence in the afternoon and was happy to hear that his urinary output continued to increase. This was by subjective reporting, as Lawrence’s Foley catheter had been removed. His white count was in normal range and his anemia was stable, if still significant. His BUN and creatinine had improved to 37 and 2.4 off dialysis. Dr. Desai ordered the removal of his hemodialysis catheter.
Hospitalist Lawrence Chua, MD came in to evaluate Lawrence for discharge home on April 13, 2018. He reviewed each day of his hospitalization for the record and noted that Lawrence had received five hemodialysis treatments. His episodes of confusion had not recurred, and psychiatry continued the antipsychotic medication as needed after an initial consult. A brain CT showed no acute intracranial disease. Physical therapy and occupational therapy worked with Lawrence during the last few days of his hospitalization, working to mobilize him and improve his stamina for a safe discharge to home self-care with only minor assistance from his family. Lawrence was discharged from the hospital that afternoon with the discharge diagnoses of “acute renal failure secondary to acute tubular necrosis and post-infectious glomerulonephritis—no evidence of acute interstitial nephritis,” “bloody diarrhea with stool positive for Shiga toxin 2,” “anemia,” “colitis,” “thrombocytopenia—improved,” “hyponatremia—improving,” “metabolic acidosis—improving,” “lower extremity swelling,” “hypotension—better with albumin and NS,” and “elevated liver function.”
Return to Deer Valley Hospital – possible pulmonary embolism
Over the next few days, Lawrence experienced some episodes of shortness of breath when he was up and about, as well as awakening at night feeling uncomfortable in his upper chest. On April 15, 2018, he returned to Deer Valley Hospital in the early afternoon, where Jennifer Prosser, DO admitted him from the emergency department after a chest CT revealed he had small bilateral pleural effusions. She thought this was consistent with compressive atelectasis and/or pneumonia. He had a small right kidney stone, minimal ascites, as well as gallstones noted on imaging. Lawrence reported he still had leg swelling, but venous duplex monitoring of his lower extremities ruled out a deep vein thrombosis. His labs showed a normal white count and stable anemia, and his renal function showed continued improvement since he was discharged on the 13th.
Dr. Prosser ordered a nuclear medicine lung V/Q scan to rule out a pulmonary embolism. Interventional radiologist Barry Sadegi, MD performed the exam and identified a “large triple-matched defect of the right lower lobe, with intermediate probability for pulmonary arterial embolism.” Dr. Prosser requested a pulmonary consultation.
Hospital Day 2
On April 16, 2018, Cristian Jiveau, MD came in for the pulmonary consultation and reviewed the imaging from the night before. He identified a number of concerns, including the CT chest that suggested right lung consolidation vs. atelectasis, as well as the V/Q scan revealing a likely pulmonary embolism. Dr. Jiveau started Lawrence on IV antibiotic therapy with Unasyn and advised that he be up and ambulating while he was hospitalized. He ordered Mucomyst[10] for renal protection prior to getting pulmonary CTA imaging to investigate the possible embolism further. Dr. Jiveau consulted with nephrology, who thought that Lawrence needed to be diuresed, but they would hold that for 24 hours after the IV contrast needed for the pulmonary CTA to avoid further renal injury.
Dr. Mumick came in for nephrology and reviewed the renal lab results done on Lawrence’s admission, noting an improvement of his serum creatinine to 1.4 that day. He observed that he had been put on a heparin drip to minimize a deep vein thrombosis and that he was slated for a CTA the next day to definitively diagnose or rule out a pulmonary embolism. He agreed with aggressive diuresis after the CTA and agreed with the Mucomyst premedication.
Hospital Day 3-4 – CTA rules out pulmonary embolism
On April 17, 2018, Lawrence underwent a pulmonary CT angiogram, which was negative for a pulmonary embolism. David Porvin, DO came in for pulmonary and noted that Lawrence had improved shortness of breath and he was being successfully diuresed after the CTA. His doctors were able to stop his heparin drip and changed it to three times daily injections for DVT prophylaxis. Lawrence continued to do well overnight, and he was initially planned to be discharged from the hospital on April 18, 2018. Ronald Allen Charles, MD evaluated him and reviewed his hospital course. After consulting with nephrology, the decision was made to keep Lawrence an extra night for continued diuresis.
Hospital Day 5 – going home
On April 19, 2018, Lawrence was doing well and had no recurrent of dyspnea. His doctors felt that his clinical presentation that led to his current admission was likely the result of fluid overload that was residual from his prolonged hospitalization for E. coli infection, acute renal failure, and hemodialysis. He was released that afternoon to outpatient follow-up. Dr. Charles gave him a prescription for a diuretic to take at home.
Home and slowly improving…
Charles reflects on his hospitalization and going home to South Dakota:
I had 5 dialysis treatments because my kidneys were not working. My sister from South Dakota had flown down and was staying at a nearby hotel. My kidneys started working again with lots of prayers from family near and far. At that point they let me go back to my daughter’s home in Phoenix for a few weeks. My wife’s sister flew down from South Dakota and helped to drive us home.
Sanford Health – Beresford Clinic
May 14, 2018, Charles presented to Sanford Health – Beresford Clinic – in Sioux Falls, South Dakota, where Judith Nelson, APRN saw him in follow-up of his hospitalization for “bloody diarrhea after eating Casear salad at a fast food restaurant.” She noted that Lawrence had just returned home to Beresford the week before. On exam, she found his lungs were clear, and his lab work that day revealed still-abnormal renal function, with a BUN and creatinine of 23 and 1.40. She made no changes to his medications (Bumex for diuresis, and hydralazine for blood pressure) and asked him to return in three months for a recheck. Lawrence returned to see NP Nelson on July 20, 2018 for unrelated blood pressure issues and chronic knee pain.
Avera Medical Group Nephrology – diagnosis CKD Stage 3
On August 15, 2018, Lawrence presented to Avera Medical Group Nephrology, where Arvin Santos, MD saw him in follow-up of acute renal failure. Dr. Santos observed that Lawrence did not have a known history of chronic kidney disease until being hospitalized the previous April with enteritis/colitis needing short term dialysis in Arizona, although a review of his records revealed microscopic hematuria in 2012. He had a longstanding history of hypertension but no diabetes.
Dr. Santos diagnosed Lawrence with acute renal failure with hematuria and proteinuria, which he thought was likely chronic kidney disease stage 3 (CKD-3). He thought that Lawrence’s serum creatinine was stable since his admission and that his current value could be his new baseline. He explained the importance of hypertension, hyperlipidemia, and blood sugar control to avoid worsening kidney disease. He advised Lawrence to avoid NSAIDs, since they could also cause kidney failure. Lawrence admitted to taking a lot of NSAIDs in the past. Dr. Santos requested lab tests to include blood testing for autoimmune disorders, as well as a renal ultrasound.
Lawrence underwent a bilateral renal ultrasound on August 26, 2018, which revealed kidney stones (calculi) that were non-obstructing, and a follow-up CT scan was ordered. On August 21, the CT scan was performed by Jonah Luzier, MD, during which he observed an increase in the size of his bilateral renal calculi. The extrarenal right renal pelvis remained mildly dilated at 17 mm which was decreased from 21 mm by comparison with prior imaging.
On September 6, 2018, Lawrence returned to see Dr. Santos and discussed that his clinical presentation laboratory analyses were consistent with a diagnosis of chronic kidney disease, stage 3 (CKD-3).[11] His serum creatinine was stable at 1.3, which he reiterated was likely his baseline. They discussed his renal CT, showing dilation of right pelvis, as well as possible hydronephrosis. Dr. Santos noted that Lawrence had seen Matthew Witte, MD at Urology Specialists Clinic in the past, who would re-consult. Dr. Santos explained the importance of hypertension, hyperlipidemia, and blood sugar control to avoid worsening kidney disease. He also explained the importance of avoiding NSAIDs since this could also cause kidney failure.
Dr. Santos advised a renal stone diet, which included but was not limited to low salt, low animal protein, low oxalate, and normal calcium dietary intake. He advised him to increase his oral fluids to achieve a urine output goal of greater than 2 liters in 24 hours. Finally, Dr. Santos addressed Lawrence’s history of gout and the need to keep his uric acid under 7 to avoid worsening renal function.
Urology Specialists Clinic
On October 22, 2018, Lawrence presented to Urology Specialists Clinic, where Dennis Thum, MD saw him in consultation for his “significant right-sided stone burden noted on CT.” He reported no current pain from his kidney stones. Dr. Thum ordered a urine culture and discussed doing a right ureteroscopy laser lithotripsy to break up the stones. After discussing the risks and benefits, Lawrence agreed to the procedure. This was done on November 9, 2018 at USC Ambulatory Services Center. He continued follow-up with Dr. Thum in December.
Aftermath
Charles reflects on his E. coli infection and how he is doing now:
It was not fun running to the bathroom every little while, and this still continues. I had to wear diapers for quite some time which is humiliating. I don’t remember a lot of what happened as they gave me a lot of pain medications. When I started dialysis I became very depressed and gave the RN’s a bad time and thought I was done for. My family had left me in the hospital and I thought I was going to be there for a long time or forever. I was very unhappy and felt like my life might be over.
Most everyone I knows was in South Dakota so I was not able to spend time with them until I was well enough to return home. I probably wasn’t the best of company myself, you tend to feel sorry for yourself in these situations, wondering how it will turn out. I am lucky my friends came to see me and support me. My sister and sister in law both flew down to Arizona were great support for both me and for my wife. My sister cheered me up and my sister in law helped us pack up to drive back home. Most of my friends are in South Dakota so I had a lot of people calling and texting me their love and support.
The doctors told me what could happen to me, to have me prepared for the worst and the best that could happen as a result of my kidney damage from contracting e coli. I am glad the worst has not happened, but I worry about the future as a result of what happened. I am hoping to get better as time goes by.
It has slowed me down a lot. When traveling anywhere, I have to be aware of where a restroom could be constantly. I have to urinate frequently because of one of the pills I now have to take to get rid of excess fluids. I have not been able to golf , I lost a lot of weight while in the hospital and it has been hard to regain my strength back.
I now have a kidney Dr. Santos, in South Dakota and was tested this past week and said I have 52-53% kidneys working at present. I have to be careful not to harm them anymore.

Lawrence looking gaunt on March 6, 2019
The causal link between Lawrence O’Conner’s E. coli O157 infection and the romaine lettuce that he consumed at Red Lobster is clear. Lawrence consumed contaminated romaine lettuce in a Caesar Salad from Red Lobster located in Peoria, Arizona on March 23, 2018.
Lawrence began to experience symptoms consistent with E. coli infection on March 26, 2018. An exposure on March 23 is consistent with an incubation period that averages 3 to 4 days for Shiga toxin-producing E. coli (STEC). A stool specimen collected on March 29, 2018 tested positive for STEC O157 and Shiga toxin at Banner Thunderbird Medical Center in Glendale, Arizona. This specimen was sent to the Arizona Department of Health Services, as Lawrence was spending time in Arizona that winter, where further genetic testing determined that Lawrence’s E. coli infection was a genetic match to the Yuma, Arizona romaine E. coli outbreak strain (PFGE pattern EXHX01.0047/ EXHA26.0626).
Given Lawrence’s infection with STEC O157, his exposure to romaine lettuce within the average STEC incubation period, and his illness during the peak of the multistate outbreak associated with Yuma, Arizona romaine lettuce, Lawrence was identified as a confirmed case in the Yuma, Arizona romaine E. coli outbreak (Outbreak ID: 1804MLEXH-1) by the South Dakota Department of Health.
____________________________________________________
[1] Reference ranges for this lab: WBC 4.0-11.0K, Hgb 13.5-17.0 g/dL, hematocrit 40-53%, platelets 130-450K, BUN 5-20 mg/dL, serum creatinine 0.5-1.30 mg/dL, AST 14-59 U/L, ALT 11-66 U/L, total bilirubin 0.0-1.3 mg/dL, CRP 0.0-9.9 mg/dL, ESR 0-20 mm/hr
[2] It is unclear in the medical record whether Lawrence was notified of the positive Shiga toxin 2 result.
[3] Cirrhosis is a chronic disease of the liver characterized by scarring of the liver with loss of normal hepatic architecture and areas of ineffective regeneration. Clinical symptoms result from loss of functioning liver cells and increased resistance to blood flow through the liver (portal hypertension). Venes, Donald. Taber’s Cyclopedic Medical Dictionary (Taber’s Cyclopedic Medical Dictionary (Thumb Index Version)) (Page 494). F.A. Davis Company. Kindle Edition.
[4] The hallmark of hemolytic uremic syndrome in the peripheral smear is the presence of schistocytes. These consist of fragmented, deformed, irregular, or helmet-shaped RBCs. They reflect the partial destruction of red blood cells (RBCs) that occurs as they traverse vessels partially occluded by platelet and hyaline microthrombi. The peripheral smear may also contain giant platelets. This is due to the reduced platelet survival time resulting from the peripheral consumption/destruction. A consumptive coagulopathy is typically not present. Nayer, Ali, and Luis M. Ortega. “Journal of Nephropathology.” Journal of nephropathology 3.1 (2014).
[5] Microangiopathic hemolytic anemia
[6] The hemolytic-uremic syndrome (HUS) is defined by the association of hemolytic anemia (low haptoglobin levels, high lactate dehydrogenase levels, and schistocytes), thrombocytopenia, and acute renal failure. Olivia Boyer and Patrick Niaudet, “Hemolytic Uremic Syndrome: New Developments in Pathogenesis and Treatment,” International Journal of Nephrology, vol. 2011, Article ID 908407, 10 pages, 2011. doi:10.4061/2011/908407
[7] Oliguria is defined as a urine output that is less than 1 mL/kg/h in infants, less than 0.5 mL/kg/h in children, and less than 400 mL daily in adults. It is one of the clinical hallmarks of renal failure and has been used as a criterion for diagnosing and staging acute kidney injury (AKI), previously referred to as acute renal failure. https://emedicine.medscape.com/article/983156-overview
[8] Risperdone is an atypical antipsychotic sometimes used to treat “ICU delirium.” While the pathophysiology of delirium is still not entirely understood, there is certainly evidence to support the hypothesis of a final common pathway of an ongoing hyperdopaminergic and hypocholinergic state perhaps triggered by oxidative stress and associated with excitotoxicity. Trzepacz PT. Is there a final common neural pathway in delirium? Focus on acetylcholine and dopamine. Semin Clin Neuropsychiatry. 2000;5(2):132–148. [PubMed]
[9] In nearly all patients, aHUS can be distinguished from TTP on the basis of an ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13) enzyme activity measurement. It is essential that aHUS and TTP be differentiated quickly, as they require markedly divergent treatments. The standard treatment for TTP is plasma exchange, a therapy that has no role for patients with a diagnosis of aHUS established by ADAMTS13 activity levels. http://www.hematologyandoncology.net/files/2013/02/ho1012_sup171.pdf
[10] Mucomyst (NAC) is the brand name for acetylcysteine, a medication ordinarily used to treat acetaminophen overdose. It is also used to loosen thick pulmonary mucus secretions, such as is seen in cystic fibrosis or COPD, as well as to prevent contrast-induced nephropathy (CIN). Although the exact mechanism responsible for the protective action of NAC from renal function deterioration remains unclear, the antioxidant and vasodilatory properties of NAC have been suggested as the main mechanisms. Jo, Sang-Ho. “N-acetylcysteine for Prevention of Contrast-Induced Nephropathy: A Narrative Review” Korean circulation journal vol. 41,12 (2011): 695-702.
[11] A person with stage 3 chronic kidney disease (CKD) has moderate kidney damage. This stage is broken up into two: a decrease in glomerular filtration rate (GFR) for Stage 3A is 45-59 mL/min and a decrease in GFR for Stage 3B is 30-44 mL/min. As kidney function declines waste products can build up in the blood causing a condition known as “uremia.” In stage 3 a person is more likely to develop complications of kidney disease such as high blood pressure, anemia (a shortage of red blood cells) and/or early bone disease. Reference: https://www.davita.com/kidney-disease/overview/stages-of-kidney-disease/stage-3-of-chronic-kidney-disease/e/4749