
According to the NICD, Aas of 26 March 2018, a total of 982 laboratory-confirmed listeriosis cases have been reported to NICD since 01 January 2017 (Figure 1). Most cases have been reported from Gauteng Province (59%, 576/982) followed by Western Cape (12%, 121/982) and KwaZulu-Natal (7%, 71/982) provinces. Cases have been diagnosed in both public (65%, 634/982) and private (35%, 348/982) healthcare sectors.Listeria monocytogenes was most commonly isolated/detected on blood culture (72%, 711/982), followed by CSF (21%, 207/982). Where age was reported (n=943), ages range from birth to 93 years (median 22 years) and 41% (404/982) are neonates aged ≤28 days (Figure 2). Of neonatal cases, 96% (389/404) had early-onset disease (birth to ≤6 days). Females account for 56% (531/950) of cases where gender is reported. Final outcome data is available for 70% (687/982) of cases, of which 28% (189/687) died.

The recall of polony has turned the tide on illnesses.

But, what about the victims, where are their stories?

 I am just not sure about this. Should a grower responsible for illnesses and deaths and the devastation of the Australian rockmelon industry be allowed to start production of rockmelon months after an outbreak?
I am just not sure about this. Should a grower responsible for illnesses and deaths and the devastation of the Australian rockmelon industry be allowed to start production of rockmelon months after an outbreak?
 Summary of Key Findings:
Summary of Key Findings: Food poisoning meets economics in this episode of the Food Chain. And it’s a toxic mix.
Food poisoning meets economics in this episode of the Food Chain. And it’s a toxic mix. “Richard Spoor, a lawyer in South Africa, has filed a $2 billion lawsuit against Tiger Brands. Nearly 70 victims and family members are part of the suit, according to William D. Marler, a Seattle-based food safety lawyer who is a consultant on the case.”
“Richard Spoor, a lawyer in South Africa, has filed a $2 billion lawsuit against Tiger Brands. Nearly 70 victims and family members are part of the suit, according to William D. Marler, a Seattle-based food safety lawyer who is a consultant on the case.”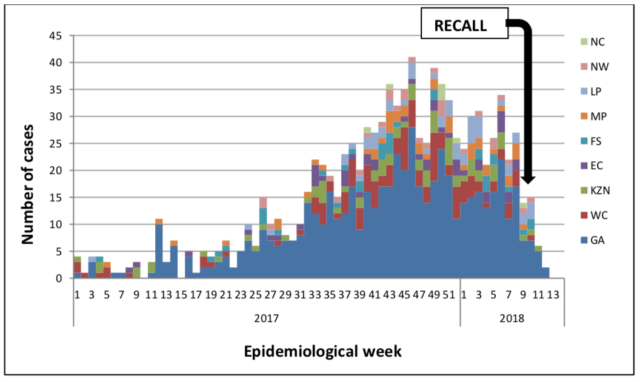

 Employees at two local Louisville, Kentucky businesses have been diagnosed with Hepatitis A.
Employees at two local Louisville, Kentucky businesses have been diagnosed with Hepatitis A. A team from the US Centers for Disease Control and Prevention (CDC) and partners in 10 states that are part of the FoodNet surveillance network reported its findings today in the latest issue of Morbidity and Mortality Weekly Report (MMWR).
A team from the US Centers for Disease Control and Prevention (CDC) and partners in 10 states that are part of the FoodNet surveillance network reported its findings today in the latest issue of Morbidity and Mortality Weekly Report (MMWR). According to the
According to the  FDA and state health and regulatory officials collected leftover dried coconut from ill people’s homes, as well as dried coconut from Natural Grocers store locations where ill people shopped and from the Natural Grocers’ Distribution Center. FDA testing identified the outbreak strain of Salmonella Typhimurium in an unopened sample of Natural Grocers Coconut Smiles Organic collected from Natural Grocers. The outbreak strain was also identified in an opened, leftover sample of Natural Grocers Coconut Smiles Organic collected from an ill person’s home.
FDA and state health and regulatory officials collected leftover dried coconut from ill people’s homes, as well as dried coconut from Natural Grocers store locations where ill people shopped and from the Natural Grocers’ Distribution Center. FDA testing identified the outbreak strain of Salmonella Typhimurium in an unopened sample of Natural Grocers Coconut Smiles Organic collected from Natural Grocers. The outbreak strain was also identified in an opened, leftover sample of Natural Grocers Coconut Smiles Organic collected from an ill person’s home.