
United State illnesses occurred between 9/6/2021 – 12/18/2021 – First recall 2/17/22
Recalled products were distributed to the following countries in addition to the United States: Australia, Bahrain, Barbados, Bermuda, Canada, Chile, China, Colombia, Costa Rica, Dominican Republic, Ecuador, Egypt, Guam, Guatemala, Hong Kong, India, Indonesia, Israel, Jordan, Kuwait, Lebanon, Malaysia, Mexico, New Zealand, Oman, Peru, Puerto Rico, Qatar, Saudi Arabia, Singapore, South Africa, Sudan, Taiwan, Thailand, United Arab Emirates, United Kingdom, and Vietnam ANI South.
FDA: Findings to date include several positive Cronobacter results from environmental samples taken by FDA at Abbott in Sturgis, Michigan facility.
FDA: A review of the Abbott ’s internal records also indicate environmental contamination with Cronobacter sakazakii.
FDA: Abbott destroyed product due to the presence of Cronobacter sakazakii.
Yesterday, the U.S. Food and Drug Administration announced it is investigating consumer complaints of Cronobacter sakazakii and Salmonella Newport infections. All of the cases are reported to have consumed powdered infant formula produced from Abbott Nutrition’s Sturgis, Michigan facility. As a result of the ongoing investigation, along with the U.S. Centers for Disease Control and Prevention and state and local partners, the FDA is alerting consumers to avoid purchasing or using certain powdered infant formula products produced at this facility.
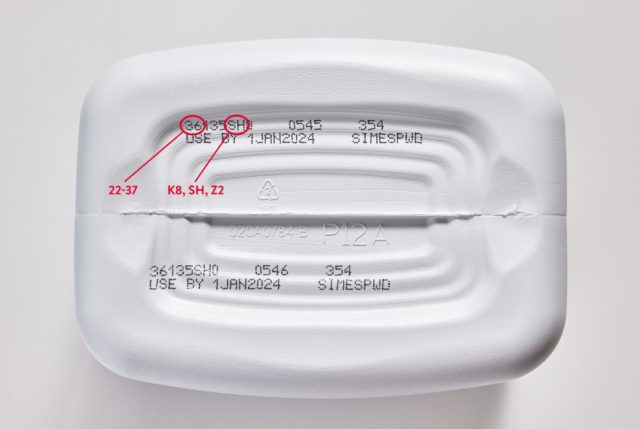
The FDA is advising consumers not to use Similac, Alimentum, or EleCare powdered infant formulas if:
- the first two digits of the code are 22 through 37; and
- the code on the container contains K8, SH or Z2; and
- the expiration date is 4-1-2022 (APR 2022) or later.
The FDA is investigating complaints of four infant illnesses from three states. All four cases related to these complaints were hospitalized and Cronobacter may have contributed to a death in one case. The FDA has initiated an onsite inspection at the facility. Findings to date include several positive Cronobacter sakazakii results from environmental samples taken by the FDA and adverse inspectional observations by the FDA investigators. A review of the firm’s internal records also indicate environmental contamination with Cronobacter sakazakii and the firm’s destruction of product due to the presence of Cronobacter.
Additional Information:
- Products made at the Sturgis, Michigan facility can be found across the U.S. and were likely exported to other countries.
- Products that do not contain the information listed above are not impacted. The FDA advisory does not include liquid formula products or any metabolic deficiency nutrition formulas. Consumers should continue to use all products not covered by the advisory.
- To date, this investigation has been associated with four illnesses (three for Cronobacter and one for Salmonella) spanning the following states: MN, OH and TX. All four cases related to these complaints were hospitalized and Cronobacter may have contributed to a death in one case.
- Cronobacter bacteria can cause severe, life-threatening infections (sepsis) or meningitis (an inflammation of the membranes that protect the brain and spine). Symptoms of sepsis and meningitis may include poor feeding, irritability, temperature changes, jaundice (yellow skin and whites of the eyes), grunting breaths and abnormal movements. Cronobacter infection may also cause bowel damage and may spread through the blood to other parts of the body.
- Parents and caregivers of infants who have used these products, and are concerned about the health of their child, should contact their child’s health care provider. If your child is experiencing any of these symptoms, you should notify your child’s healthcare provider and seek medical care for your child immediately.
- Salmonella are a group of bacteria that can cause gastrointestinal illness and fever called salmonellosis. Most people with salmonellosis develop diarrhea, fever and abdominal cramps. More severe cases of salmonellosis may include a high fever, aches, headaches, lethargy, a rash, blood in the urine or stool, and in some cases, may become fatal.
- Parents and caregivers should never dilute infant formula and should not make or feed homemade infant formula to infants.
- If your regular formula is not available, contact your child’s healthcare provider for recommendations on changing feeding practices.
The FDA is continuing to investigate and will provide additional consumer safety information when it becomes available.


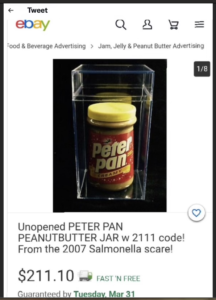 A week ago one of my food safety followers on Twitter sent me this photo that was apparently circulating offering for sale on eBay a product that was recalled over a decade ago. They asked if it was legal for someone to sell a recalled food product.
A week ago one of my food safety followers on Twitter sent me this photo that was apparently circulating offering for sale on eBay a product that was recalled over a decade ago. They asked if it was legal for someone to sell a recalled food product.
")
 As of January 28, there have been 14 laboratory-confirmed cases of
As of January 28, there have been 14 laboratory-confirmed cases of 

 Over 200 died, many were the young and the unborn who will never turn 4.
Over 200 died, many were the young and the unborn who will never turn 4.





















 And, then the 2018 romaine lettuce E. coli outbreak struck, sickening hundreds in the United States and Canada with dozens suffering from acute kidney failure with five reported deaths. Once again, the Wellton Irrigation Canal was the focus of attention in the “Memorandum to File on the 2018 Environmental Assessment”:
And, then the 2018 romaine lettuce E. coli outbreak struck, sickening hundreds in the United States and Canada with dozens suffering from acute kidney failure with five reported deaths. Once again, the Wellton Irrigation Canal was the focus of attention in the “Memorandum to File on the 2018 Environmental Assessment”:



 The Montgomery County Office of Public Health (OPH) announced today the temporary closure of Gino’s Ristorante & Pizzeria in West Norriton in relation to a
The Montgomery County Office of Public Health (OPH) announced today the temporary closure of Gino’s Ristorante & Pizzeria in West Norriton in relation to a 




